RUSSELL H. CASHIN
Title: CANNABIS IS ALWAYS THERAPEUTIC
Area:
Country:
Program: Doctor of Philosophy
Available for Download: Yes
View More Student Publications Click here
For more information on the AIU's Open Access Initiative, click here.
INTRODUCTION
There is a movement sweeping through the United States as well as in many other countries around the legal status of the plant known as cannabis. This momentum is so powerful that some of the most conservative states are beginning to pass medical cannabis legislation even though the cannabis plant and many of its components remain, as of this writing, a Schedule 1 drug at the federal level.
There currently exists an ongoing debate over what constitutes “medical” cannabis verses what is often labeled “recreational” or “adult use.” The apprehension over the idea of “recreational cannabis” is so powerful that it actually seems to be slowing cannabis reform in some states and hindering the implementation and distribution of the cannabis “medicine” even after medical cannabis laws have been passed.
As the science and industry of cannabis is progressing there appears to be an idea emerging that cannabis may in fact always be therapeutic even when it is thought by the individual to be ingested for “recreational” or “creative” purposes. There have been very few if any studies, descriptive or otherwise, that touch on this notion. Given that it is now understood that the endocannabinoid system or ECS may be the largest neurotransmitter system network in the human brain, we must look at the underlying psychological and therapeutic effects of cannabis that may be occurring even when the user is consciously unaware of them.
Dr. Dustin Sulak, an osteopathic physician and Diplomat of the American Academy of Cannabinoid Medicine, states that the Endocannabinoid System is “perhaps the most important physiologic system involved in establishing and maintaining human health” (Sulak, 2015). He also describes humans as essentially a single-unit organism that require a well-balanced internal system in order to grow and function optimally. He further indicates that an imbalanced state of
homoeostasis can lead to health problems ranging from minor headaches and emotional issues to more serious life-threatening conditions such as cancer (Sulak, 2015).
There have been at least 25,000 articles on cannabis, cannabinoids and the ECS published in peer-reviewed medical journals since 1995. It is becoming increasingly understood that the Endocannabinoid System helps to regulate important processes that maintain an individual’s homoeostasis by activating cannabinoid receptors known as CB1 and CB2 in the central nervous and peripheral nervous systems in the human body. Restoration of this homoeostasis is obtained through the process of eating a healthy diet, receiving sufficient sleep, exercising and additionally consuming “whole plant” cannabis in whatever form is ideal for the individual situation (Sulak, 2015).
It is time to move towards a more in-depth understanding of the beneficial impact of the numerous components of cannabis on the human condition and how it improves the overall sense of wellness. Nevertheless, in order to understand cannabis’ demonization because of social prejudices and its rediscovery as the medicine of the 21st century we must look to history, the scientific makeup of the plant, and its medicinal use both in ancient and modern times.
Background
In order to fully appreciate the significance of cannabis and the endocannabinoid system it is necessary to cover, at least briefly, what cannabis is and its long relationship and history in human culture.
The Plant
Cannabis is a plant that is comprised of related subspecies that have often been lumped together. Cannabis Sativa is referred to as Hemp when it contains negligible amounts of THC. When the THC levels are higher than the arbitrarily defined .3% “legal” limit, Cannabis Sativa is often inaccurately referred to as Marijuana. When observing the plant, the typical Sativa subspecies tend to have skinnier leaves that are concentrated at the top and can grow up to 20 ft. in height (see illustration 1.1). Hemp Sativa is considered a non-psychotropic plant cultivar containing less than .3% of THC (the most active psychotropic component) and is primarily used in manufacturing products such as oil, cloth and fuel. Cannabis Sativa (marijuana) typically contains anywhere from 5-20% of THC, and some premium cultivars contain more. There is a another subspecies of the plant known as Cannabis Indica (see illustration 1.2) which is typically shorter than Cannabis Sativa and is much broader leafed, but also contains levels of THC similar to the Sativa. There is a third less common plant known as Cannabis Ruderalis. All subspecies contain various amounts of another significant cannabinoid known as CBD depending on the plant genetics.
In recent times, so much hybridization has occurred between the various subspecies, that it is questioned if there are any true pure sativa, indica or ruderalis cultivars. It is probably more accurate to describe cannabis in terms of the dominant characteristics of each plant such as sativa or indica dominant. Ruderalis is primarily for creating auto-flowering varieties of the plant.
History of Cannabis
Based on recent research that was conducted at the University of Toronto (2018), the two most distinct compounds known as THC and CBD did not always exist in the plant we now call
cannabis. According to that study, millions of years ago ancient viruses may have colonized the plant's genome and hastened a process that changed the plant’s DNA.
Researchers believe that these ancient viruses may have accelerated an evolutionary process resulting in a single enzyme gene in cannabis mutating into two (Laverty et al., 2018). This eventually gave us the two most well-known cannabinoids, THC and CBD. This change probably led to the ancient cannabis plant splitting into chemically distinct types, and humans then selected plants with desired characteristics eventually leading to the hybrid cultivars we have today.
According to a published review by Barney Warf, professor of geography at the University of Kansas, cannabis use among humans originated thousands of years ago in Asia and was widely used as a medicine as well as for spiritual purposes (Warf, 2014). Professor Warf points out that the Vikings and medieval Germans used cannabis for relieving pain during childbirth as well as for toothaches.
Cannabis is thought to have developed on the steppes of Central Asia, specifically in the regions that are now Mongolia and southern Siberia, according to Warf. The human history of cannabis use appears to go back as far as 12,000 years, which places the plant among humanity's oldest cultivated crops (Abel, 1980).
Burned cannabis seeds have been found in kurgan burial mounds in Siberia dating back to 3,000 B.C., and in some of the tombs of noble people buried in Xinjiang region of China and Siberia around 2500 B.C. have included large quantities of mummified cannabis.
Both hemp and cannabis were widely used in ancient China with the first record of the plant’s medicinal use dating to around 4000 B.C. The herb was used for instance as an anesthetic during surgery, and stories say it was even used by the Chinese Emperor Shen Nung in 2737
B.C. (although it is still debated whether Shen Nung was a real or a mythical figure since the first emperor of a unified China was born much later than the supposed Shen Nung.)
From China, coastal farmers brought the cannabis plant to Korea in around 2000 B.C. or perhaps even earlier (Nelson, 1993). Cannabis arrived in the South Asian subcontinent between 2000 B.C. and 1000 B.C., when the Aryans invaded the region. The plant became widely used in India, where it was celebrated as one of "five kingdoms of herbs ... which release us from anxiety" according to one of the ancient Sanskrit Vedic poems whose name translates into the "Science of Charms."
Cannabis then arrived in the Middle East between 2000 B.C. and 1400 B.C., and the Scythians, a nomadic Indo-European group, likely used it there. The Scythians also likely carried the plant into southeast Russia and Ukraine, according to Professor Warf's report. Germanic tribes brought the plant into Germany and cannabis went from there to Britain during the 5th century with the Anglo-Saxon invasions. Cannabis seeds have also been found in the remains of Viking ships dating to around the mid-ninth century.
Over the next several centuries, cannabis migrated to various regions of the world, traveling through Africa, reaching South America in the 19th century and being carried north afterwards.
After a long journey throughout the pre-modern and modern worlds, cannabis finally came to the United States at the beginning of the 20th century. It arrived in the southwest United States from Mexico with the immigrants who fled that country during the Mexican Revolution of 1910-1911. In fact, many early prejudices against cannabis were actually thinly veiled racist fears of these immigrant smokers, often promulgated by reactionary newspapers. Professor Warf writes, "Mexicans were frequently blamed for smoking marijuana, property crimes, seducing
children and engaging in murderous sprees" (Warf, 2014). In fact, prior to 1910, “marijuana” did not exist as a word in American culture. Rather, the term “cannabis” was most often used in reference to the medicines and remedies for common household ailments. In the early 1900’s the pharmaceutical companies of Meyer’s Squib and Eli Lilly actually included cannabis and cannabis extracts in many of their medicines.
In 1930, the Great Depression had just hit the United States, and Americans were searching for someone to blame. Due to the influx of immigrants (particularly in the South) and the rise of “suggestive” jazz music, many white Americans began to treat cannabis (and, arguably, the Blacks and Mexican immigrants who consumed it) as a foreign substance intended to corrupt the minds and bodies of “low-class” individuals.
Harry Anslinger became the first commissioner of the Federal Bureau of Narcotics (FBN) in 1930 and undertook multiple efforts to make cannabis illegal in all states. It would not be an overstatement to say that Harry Anslinger was one of the primary individuals responsible for creating the stigma surrounding cannabis. It is Anslinger who launched a vigilant campaign against the plant that would hold steady for the three decades he remained in office.
We now know that Anslinger’s efforts with the Bureau of Narcotics were the reason “marijuana” became a word known by Americans all over the country. When making public appearances and creating propaganda films such as Reefer Madness, Anslinger specifically used the term “marijuana” when campaigning against the plan, adding to the development of the herb’s new “foreign” identity.
In 1937, the Marijuana Tax Act put cannabis under the regulation of the Drug Enforcement Agency, criminalizing possession of the plant throughout the country. (The plant was actually first outlawed in Utah in 1915, but by 1931 it was illegal in 29 states.)
In the early 1970’s, a very paranoid President Richard Nixon launched America’s “war on pot” by lumping marijuana, homosexuality, Jews and “Commies” into one grand conspiracy. Even after reviewing all the evidence, Nixon’s own appointed presidential commission had recommended that marijuana use should not be a criminal offense under either state or federal law. However, Nixon himself, based on his zealous personal preferences, overruled the commission's research and recommendation of cannabis legalization, further dooming marijuana to its current prohibited status federally.
The idea that this is an evil drug is a very recent creation and the fact that it is illegal is a "historical anomaly," according to Professor Warf (Warf, 2014). In actuality, cannabis has been legal in many regions of the world for most of its history and its illegal status is primarily the result of racial prejudice and a collective social class bigotry.
The Endocannabinoid System
Discovered in 1992 by Raphael Mechoulam and NIMH researchers William Devane and Dr. Lumir Hanus, the Endocannabinoid System (ECS) is a group of endogenous cannabinoid receptors located in the mammalian brain and throughout the central and peripheral nervous systems. Known as "the body’s own cannabinoid system", the Endocannabinoid System is involved in a variety of physiological processes including appetite, pain-sensation, mood and memory.
Two primary endocannabinoid receptors have been identified: CB1 and CB2. The CB1 receptors are found predominantly in the brain and nervous system, as well as in peripheral organs and tissues, and are the main molecular target of the endocannabinoid anandamide and its mimetic phytocannabinoid THC. One other main endocannabinoid is 2-Arachidonoylglycerol (2-AG) which is active at both of these primary cannabinoid receptors, along with its own mimetic
phytocannabinoid CBD or cannabidiol. CBD2 receptors are also found throughout the body in the immune cells. In other words, it is because of this endocannabinoid system that molecules from the cannabis plant can influence human physiology.
The endocannabinoid system or ECS helps to control every physiological system in the human body.
Yet despite the importance of the ECS, knowledge continues to be quite limited among American physicians and the public. The endocannabinoid system allows individual cells in the body to “talk” to each other by permitting them to share information. The endocannabinoid system is arguably the largest neural network in the brain and coordinates the vital flow of inputs and outputs of information between and within cells throughout the entire human body.
We know that a breakdown in the endocannabinoid system communication disrupts this information flow, which can result in disease or death. The endocannabinoid system is one of the main mechanisms all mammals use to keep themselves in physiochemical balance called homeostasis and subsequently free of disease.
In humans, for example, after a head injury, stroke or other physiological stressor, the body raises its own endocannabinoid levels for protection. This mobilizes the biological response to the injury, reduces harm, and promotes healing. Low levels of the chemicals known as anandamide and 2-AG in the endocannabinoid system are associated with migraine, IBS, fibromyalgia, PTSD, infertility, complex regional pain syndrome and liver fibrosis, as well as many other diseases. In fact, several studies exist that indicate the therapeutic use of the mimetic phytocannabinoids such as THC and CBD found in the cannabis plant reduces the harm caused by the imbalances that occur in our bodies due to stress and chronic disease as well as those that increase due to aging.
OBJECTIVE
The endocannabinoid system is critical in bringing the organism back into homeostasis from a crisis or stress response. With this knowledge about the function of the ECS, then it could very well be inferred that the ingestion of cannabis or its extracts may provide, at all times, a level of medical or therapeutic effect regardless of the conscious or believed reason for its use. This has been postulated as being the case (Macris, 2015), but has not been fully explored. At the very least the current science provides evidence of the use of cannabis for anxiety, depression, insomnia, PTSD, epilepsy, pain, cancer, concussions, fibromyalgia, arthritis, amyotrophic Lateral Sclerosis (ALS), asthma, diabetes, lupus, autism, glaucoma, Parkinson’s disease and Crohn’s disease.
The aims of this study are to explore the use of cannabis among adults and examine the association between the specified reasons for the use of cannabis either for therapeutic or non-therapeutic use, and to evaluate the self-reported assessment of effectiveness for the condition(s) or other reason(s) as described. Additional aims are to determine whether the individual ailment(s) have improved with use and if cannabis has instilled an expanded sense of well-being in the individual. The overall hypothesis is that cannabis use offers a therapeutic or medicinal benefit since this homeostasis is the tendency of the physiological system to maintain internal stability. In addition, cannabis should advance the individual’s sense of well-being to an observable level that should be revealed in a self-reporting questionnaire. Further, with a generally enhanced psychological equilibrium it would be additionally anticipated that there is a greater overall sense of improved health, even if the underlying condition itself is not completely healed.
METHODS
A written descriptive questionnaire was utilized along with two case study follow-up evaluations drawn from the participants of the primary survey. The additional case histories are included to provide additional related data given the small sample size of the primary descriptive study.
Design and Sample
Data for the present study was gathered from an online written questionnaire called the “Cannabis Users Survey – A Descriptive Study” that was adapted from an earlier abandoned project. Promotion of the survey included direct contact, word of mouth, and social media to over 3000 potential participants. The survey employed is an internet-based custom written questionnaire and participants were invited to contribute voluntarily without any offer of compensation. Demographics and personal data were gathered to the extent needed in order to provide follow-up contact for the chosen case studies. Only adults over the age of 18 were invited to take the survey although caregivers of adult patients were included should an individual be unable to respond online due to physical or other limitations. The participants completed the questionnaire at their convenience and the amount of time to fill out the questionnaire was estimated to be less than 30 minutes. The survey was promoted for a duration of three months from August to October in 2018, but users were allowed to respond for an additional three months.
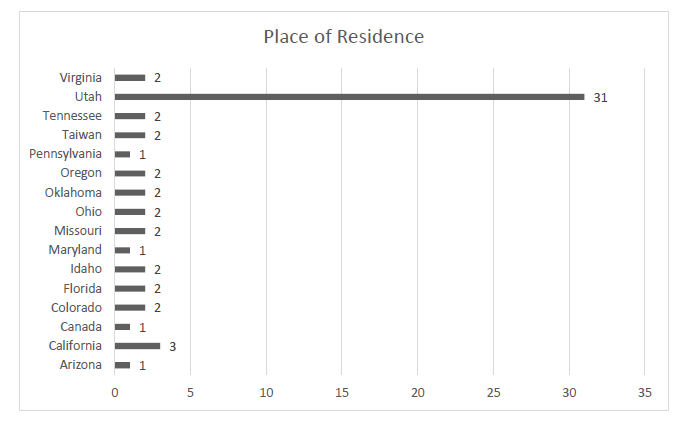
There are a total of 58 participants that chose to reply and are split evenly by sex with exactly 29 male and 29 female respondents. The geographic distribution is skewed favoring the local population with 31 or 53.45% of the responses from within the state of Utah. There were 24 responses or 41.38% from locations outside of Utah, but from within the United States. There are two (3.45%) participants answering from Taiwan and one response from Canada. See Table 1.1 for details.
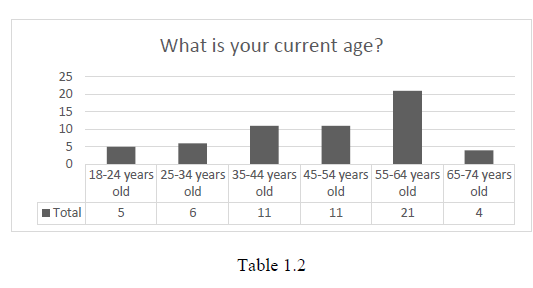
 Interestingly, the leading number of responses came from participants who are older with the largest group in the 55-64 y/o at 36.21% and the second largest tied in the 45-54 and 35-44 y/o ranges at 18.97% each. The largest number of users in the survey were individuals over 55 years of age, at 43.10%. This is likely due to the small sample size, but may also be attributed to the recent increased use of Cannabis by more than 70 percent for those over 50 years of age between 2006 and 2013 as reported in Gerontology and Geriatric Medicine (Lloyd & Striley, 2018). See table 1.2 for details.
Interestingly, the leading number of responses came from participants who are older with the largest group in the 55-64 y/o at 36.21% and the second largest tied in the 45-54 and 35-44 y/o ranges at 18.97% each. The largest number of users in the survey were individuals over 55 years of age, at 43.10%. This is likely due to the small sample size, but may also be attributed to the recent increased use of Cannabis by more than 70 percent for those over 50 years of age between 2006 and 2013 as reported in Gerontology and Geriatric Medicine (Lloyd & Striley, 2018). See table 1.2 for details.
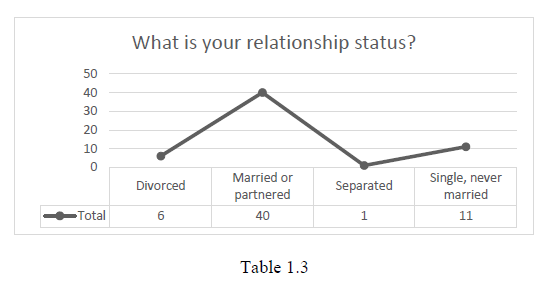
 In terms of relationship status, 69% of the participants are individuals who are married or partnered. The remaining percentages are those who declared to be single at 19%, divorced at 10.3% and separated, but not divorced at 1.7%. For the graph of these results, see Table 1.3.
In terms of relationship status, 69% of the participants are individuals who are married or partnered. The remaining percentages are those who declared to be single at 19%, divorced at 10.3% and separated, but not divorced at 1.7%. For the graph of these results, see Table 1.3.
 If we look at the educational demographic data, it is consistent with the national averages as of 2018 (Statistical Atlas, 2018). We can see this if we combine the total numbers by those who have a bachelor’s degree or higher as compared those with a high school diploma or no diploma at all. The national averages are 38.5% with a Post-Secondary Degree, 48.5% with a High School Diploma and 13% with no diploma, while the data from the cannabis study is comparable with 37.9% holding a Post-Secondary Degree, 51.7% with a High School Diploma, and 5.2% having no diploma. The individual data for each education level are show in Table 1.4.
If we look at the educational demographic data, it is consistent with the national averages as of 2018 (Statistical Atlas, 2018). We can see this if we combine the total numbers by those who have a bachelor’s degree or higher as compared those with a high school diploma or no diploma at all. The national averages are 38.5% with a Post-Secondary Degree, 48.5% with a High School Diploma and 13% with no diploma, while the data from the cannabis study is comparable with 37.9% holding a Post-Secondary Degree, 51.7% with a High School Diploma, and 5.2% having no diploma. The individual data for each education level are show in Table 1.4.
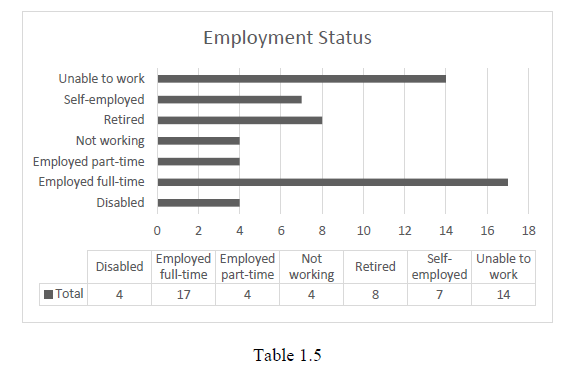
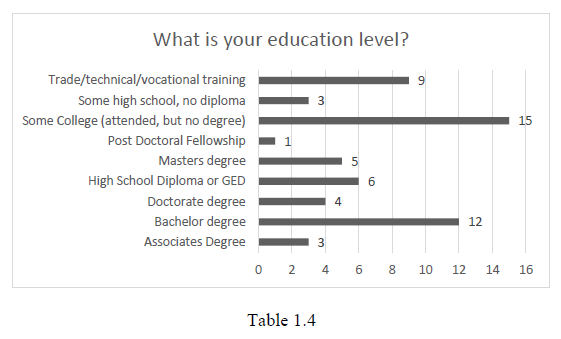 In terms of the employment status of the study participants, if we look at the overall employment rates, 48.28% are employed with 29.3% holding full-time work, 12.1% are self-employed and 6.9% are working part-time. This is lower than the national average of 58.4% (Statistical Atlas, 2018), but may be due to a 31.04% of individuals in the population sample being disabled and/or unable work with another 13.79% who are retired and the remaining 6.9% not working for other reasons that went undeclared. See Table 1.5 for the details.
In terms of the employment status of the study participants, if we look at the overall employment rates, 48.28% are employed with 29.3% holding full-time work, 12.1% are self-employed and 6.9% are working part-time. This is lower than the national average of 58.4% (Statistical Atlas, 2018), but may be due to a 31.04% of individuals in the population sample being disabled and/or unable work with another 13.79% who are retired and the remaining 6.9% not working for other reasons that went undeclared. See Table 1.5 for the details.
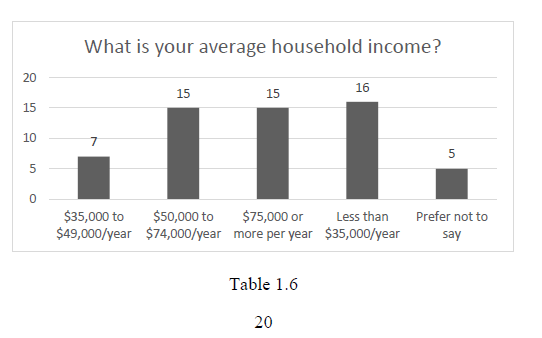
 In terms of income, a range of annual income levels was requested and 8.62% of the study participants preferred not to answer. Of the participants who did answer 27.59% fell in the lowest income of under $35,000/year, 12.07% were in the $35,000-$49,000 range. The remaining two income ranges were equally divided with 25.86% each in the $50,000-$74,000 and $75,000 or more income categories respectively. See Table 1.6.
In terms of income, a range of annual income levels was requested and 8.62% of the study participants preferred not to answer. Of the participants who did answer 27.59% fell in the lowest income of under $35,000/year, 12.07% were in the $35,000-$49,000 range. The remaining two income ranges were equally divided with 25.86% each in the $50,000-$74,000 and $75,000 or more income categories respectively. See Table 1.6.
 Study Measures
Study Measures
The custom written questionnaire that was developed consists of a broad range of questions related to the use of cannabis both by the type of plant subspecies and by the two leading and most researched active cannabinoids, THC and CBD. Five questions regarded the voluntary nature of the study and included personal information with one question considered as optional and another seven questions for demographics. Twenty-six of the questions covered the following areas; cannabis use, medical condition whether related to physical illness (cancer, chronic pain, epilepsy, glaucoma, Parkinson’s, etc.) and/or mental health (anxiety, depression, PTSD, etc.), non-medical use reasons, methods of ingestion, dosages, tolerance, side effects, overall experience and general satisfaction. Two additional questions presented the participant the opportunity to be selected for a follow-up interview and one final open-ended question for any relevant history or description of condition not otherwise covered in the non-open ended questions.
Given the number of potential responses, the sample size was considerably smaller than expected, which dictated the use of the case studies. Two participants were selected from the descriptive survey for a more in-depth case history of cannabis use.
RESULTS
Because the survey was originally created for another study that was dropped and then adapted for cannabis, some of the questions are not relevant to this thesis. In addition, other questions had numerous possible answers resulting in more responses than the total number of study participants or are duplicated. Consequently, survey questions 16, 17, 29 and 30 (see Appendix D) have been excluded from the data results for these reasons.
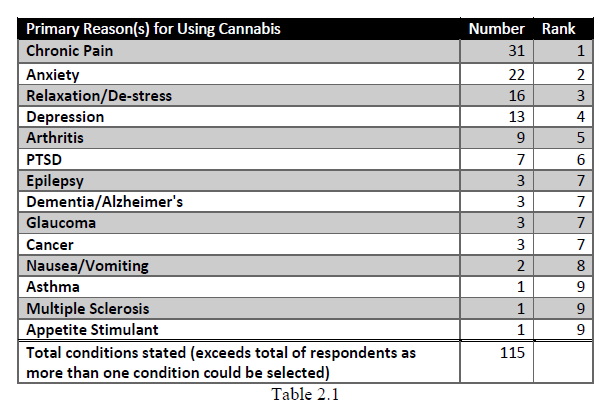
While there are only 58 participants in the descriptive study, the participants could select multiple primary reasons for cannabis use covering most of the possible conditions being treated. Rather than list all the likely combinations with the additional secondary and third reasons, the top primary conditions are ranked from the highest to lowest number of responses. The most common condition treated with cannabis in this study is pain at 31 responses with anxiety at 22 responses, relaxation/de-stress at 16, depression at 13, arthritis at nine, and PTSD at seven.
When we evaluate the condition(s) as a percentage of the total number of participants 53.45% reported pain as a primary condition being treated with cannabis, followed by anxiety at 38.8%, de-stress/relax at 27.5%, depression at 22.4%, arthritis at 15.5% and PTSD at 12%. The full list of conditions as reported in the survey may be found in table 2.1.
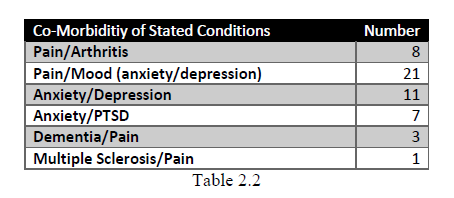
 With the number of conditions reported, a high association is apparent between pain and mood as well as other reported ailments. There appears to be a very high correlation with 67.74% of those with pain also reporting anxiety or depression. Of those who reported suffering from anxiety, almost a third (27%) or seven individuals also indicated comorbidity with PTSD. There are 11 persons that indicated comorbidity between anxiety and depression, and arthritis was associated with pain in eight individuals. Three mentioned dementia and pain together in the response, and the one person with MS also indicated using cannabis for pain. Table 2.2 shows the conditions for which comorbidity is identified.
With the number of conditions reported, a high association is apparent between pain and mood as well as other reported ailments. There appears to be a very high correlation with 67.74% of those with pain also reporting anxiety or depression. Of those who reported suffering from anxiety, almost a third (27%) or seven individuals also indicated comorbidity with PTSD. There are 11 persons that indicated comorbidity between anxiety and depression, and arthritis was associated with pain in eight individuals. Three mentioned dementia and pain together in the response, and the one person with MS also indicated using cannabis for pain. Table 2.2 shows the conditions for which comorbidity is identified.
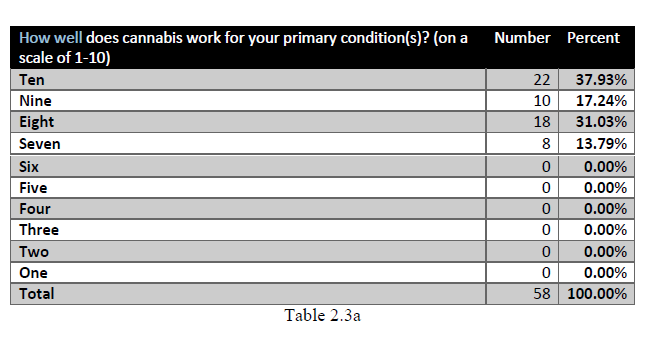
 When asked to assess how well cannabis is treating their primary condition a Likert scale from 1-10 was used with ten indicating excellent. Twenty-two respondents gave cannabis 10 out of 10. Ten individuals gave a 9 out of 10, with 18 an 8 out of 10 and eight rating cannabis a 7 out of 10. The answers with the total percentages are shown in table 2.3a.
How well
When asked to assess how well cannabis is treating their primary condition a Likert scale from 1-10 was used with ten indicating excellent. Twenty-two respondents gave cannabis 10 out of 10. Ten individuals gave a 9 out of 10, with 18 an 8 out of 10 and eight rating cannabis a 7 out of 10. The answers with the total percentages are shown in table 2.3a.
How well
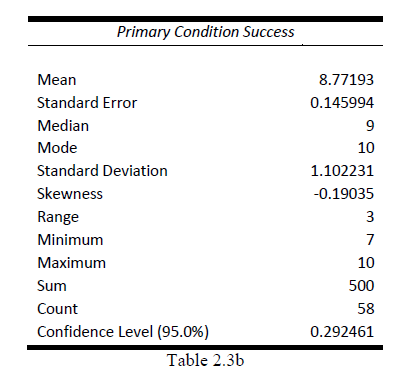
 With the previous question, an additional descriptive analysis was performed to determine the mean, standard error, standard deviation and the confidence level at 95%. The data clearly shows a mean of 8.77 (on the 1-10 scale), median of 9 and mode of 10, a standard deviation of 1.1 and a confidence level of .292. Table 2.3b offers the complete data analysis.
With the previous question, an additional descriptive analysis was performed to determine the mean, standard error, standard deviation and the confidence level at 95%. The data clearly shows a mean of 8.77 (on the 1-10 scale), median of 9 and mode of 10, a standard deviation of 1.1 and a confidence level of .292. Table 2.3b offers the complete data analysis.
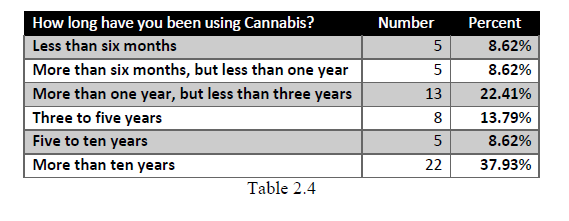
 To determine the overall experience of the survey participants have when it comes to using cannabis a question was included asking, “How long have you been using Cannabis?” The largest number of the respondents or 37.93% indicated using cannabis for “more than ten years” and in the comment section, many of those indicated having a much longer experience with cannabis, sometimes spanning decades. The second largest group were those with “more than one year, but less than three years” of experience with 22.41% answering. The remaining three groups of “five to ten years”, “more than six months, but less than one year” and “less than six months” all tied at five responses each or 8.62%. The data is shown in table 2.4.
To determine the overall experience of the survey participants have when it comes to using cannabis a question was included asking, “How long have you been using Cannabis?” The largest number of the respondents or 37.93% indicated using cannabis for “more than ten years” and in the comment section, many of those indicated having a much longer experience with cannabis, sometimes spanning decades. The second largest group were those with “more than one year, but less than three years” of experience with 22.41% answering. The remaining three groups of “five to ten years”, “more than six months, but less than one year” and “less than six months” all tied at five responses each or 8.62%. The data is shown in table 2.4.
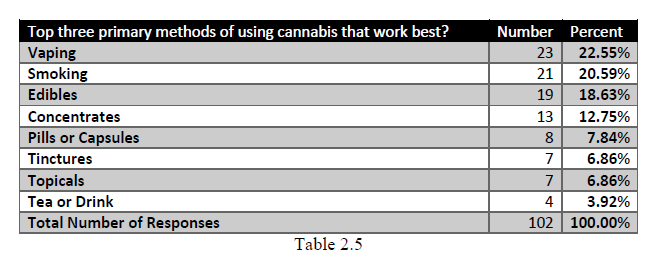
 A question was included about the top three primary methods of ingestion to gain some overall understanding of what users find helpful. Individual data is not tied to specific condition(s). Vaping took the top position with 22.55% preferring this method just ahead of smoking at 20.59%. Taken together at 43.14%, clearly these are the most preferred methods over all others. This infers that many individuals likely favor these methods due to the ease and fast acting efficacy they provide. The edibles and concentrates also rated significantly at 18.63% and 12.75% respectively. Pills, tinctures, and topicals all came well under 10% each with teas or drinks at the bottom at 3.92% usage. Table 2.5 show the individual data responses.
A question was included about the top three primary methods of ingestion to gain some overall understanding of what users find helpful. Individual data is not tied to specific condition(s). Vaping took the top position with 22.55% preferring this method just ahead of smoking at 20.59%. Taken together at 43.14%, clearly these are the most preferred methods over all others. This infers that many individuals likely favor these methods due to the ease and fast acting efficacy they provide. The edibles and concentrates also rated significantly at 18.63% and 12.75% respectively. Pills, tinctures, and topicals all came well under 10% each with teas or drinks at the bottom at 3.92% usage. Table 2.5 show the individual data responses.
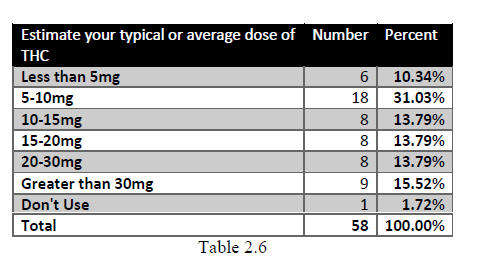
 Determining the average dose of THC and or CBD is most challenging with smoking or vaping since much of the medicine is lost in the heating process so respondents were asked to estimate based on standard charts. At best, these dosages are approximated without any information about the individual plant cultivar or cannabis product used. In addition, only THC and CBD amounts were requested since these the most commonly researched cannabinoids and the amounts are often listed on the packaging of cannabis products sold at dispensaries within a usual 15% legally allowed variance.
Table 2.6 shows the estimated THC usage and is listed below, but the typical and most common dosage was in the 5-10mg range, which is considered an average recommended dose for many of the cannabis products currently available in dispensaries.
Determining the average dose of THC and or CBD is most challenging with smoking or vaping since much of the medicine is lost in the heating process so respondents were asked to estimate based on standard charts. At best, these dosages are approximated without any information about the individual plant cultivar or cannabis product used. In addition, only THC and CBD amounts were requested since these the most commonly researched cannabinoids and the amounts are often listed on the packaging of cannabis products sold at dispensaries within a usual 15% legally allowed variance.
Table 2.6 shows the estimated THC usage and is listed below, but the typical and most common dosage was in the 5-10mg range, which is considered an average recommended dose for many of the cannabis products currently available in dispensaries.
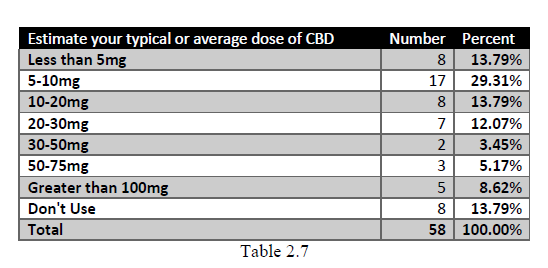
 With CBD, the most common dose was also in the 5-10mg range with less than a 2-point difference from the most common THC dosage. Table 2.7 shows the breakdown as reported in the survey.
With CBD, the most common dose was also in the 5-10mg range with less than a 2-point difference from the most common THC dosage. Table 2.7 shows the breakdown as reported in the survey.
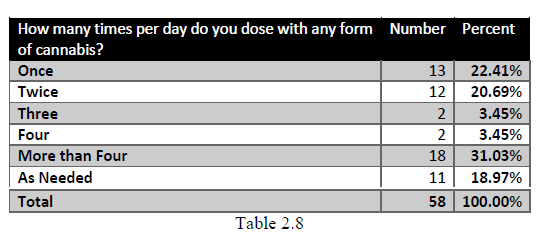
 The number of times per day individuals dose is indicated in Table 2.8. Most respondents indicated dosing more than four times a day at 31.03%. Once, twice and “as needed” came in at 2nd, 3rd and 4th respectively. The least common daily doses was three and four times per day at 3.45% each.
The number of times per day individuals dose is indicated in Table 2.8. Most respondents indicated dosing more than four times a day at 31.03%. Once, twice and “as needed” came in at 2nd, 3rd and 4th respectively. The least common daily doses was three and four times per day at 3.45% each.
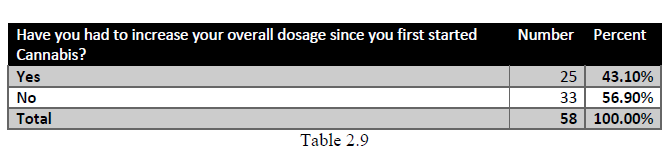
 This next question is important to determine if a rise in dosing from the start was occurring. Less than ½ needed to increase cannabis with 25 or 43.10% doing so. The majority of individuals or 56.9% did not need to increase dosing. The responses for this question are found in Table 2.9.
This next question is important to determine if a rise in dosing from the start was occurring. Less than ½ needed to increase cannabis with 25 or 43.10% doing so. The majority of individuals or 56.9% did not need to increase dosing. The responses for this question are found in Table 2.9.
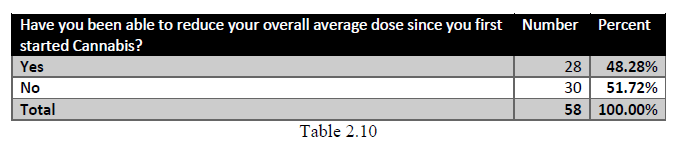
 This next question relates to the previous one in ascertaining whether individuals were able to decrease their dose to manage their condition since starting cannabis with 28 or 48.28% indicating they were able to lower the overall dose. This is nearly ½ of all respondents. The answers for this question are shown in Table 2.10.
This next question relates to the previous one in ascertaining whether individuals were able to decrease their dose to manage their condition since starting cannabis with 28 or 48.28% indicating they were able to lower the overall dose. This is nearly ½ of all respondents. The answers for this question are shown in Table 2.10.
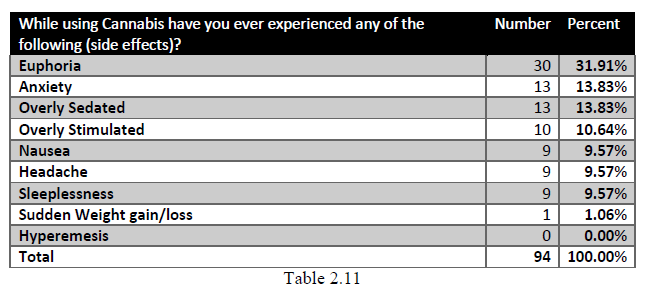
 When using cannabis, one of the areas of discussion often involves potential side effects. It is not surprising that the most common effect is euphoria with 30 affirmative responses or 31.91%. Anxiety came in the number two position and being overly sedated came in third. No one claimed “cannabis hyperemesis” as a side effect even for those who have been long-term users although this is a rare condition and may actually be the result of Azadirachtin contamination (Ago, 2018). Because it is possible to have more than one side effect for any given type or amount of cannabis, the total responses are greater than the number of participants. The entire list by the number of responses and percentage is shown in Table 2.11.
When using cannabis, one of the areas of discussion often involves potential side effects. It is not surprising that the most common effect is euphoria with 30 affirmative responses or 31.91%. Anxiety came in the number two position and being overly sedated came in third. No one claimed “cannabis hyperemesis” as a side effect even for those who have been long-term users although this is a rare condition and may actually be the result of Azadirachtin contamination (Ago, 2018). Because it is possible to have more than one side effect for any given type or amount of cannabis, the total responses are greater than the number of participants. The entire list by the number of responses and percentage is shown in Table 2.11.
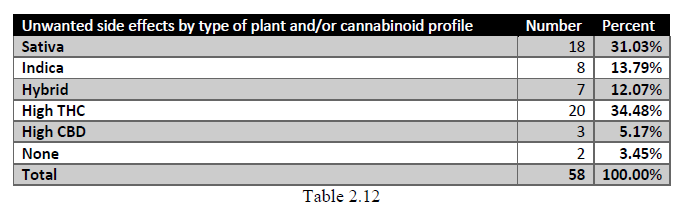
 It is also important to get some measurement around the type of plant or cannabinoid used when considering side effects. The number one plant correlated with side effects is sativa or sativa dominant cultivars with 31.03% listing this as a primary factor. The most common component of cannabis, THC came in at number one with 34.48% indicating side effects with products containing high-levels of THC. The question did not evaluate which of the side effects was most present with either the Sativa cultivar or the High THC so a correlation is not possible.
It is also important to get some measurement around the type of plant or cannabinoid used when considering side effects. The number one plant correlated with side effects is sativa or sativa dominant cultivars with 31.03% listing this as a primary factor. The most common component of cannabis, THC came in at number one with 34.48% indicating side effects with products containing high-levels of THC. The question did not evaluate which of the side effects was most present with either the Sativa cultivar or the High THC so a correlation is not possible.
The complete data is shown in Table 2.12.
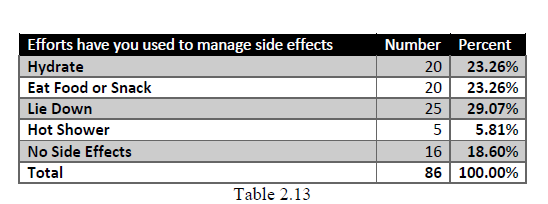
 To gain some insight into how individuals manage side effects a question was asked regarding the most common methods used. Based on the data 18.6% of participants do not have side effects at all. Lying down came as the primary method with hydration and eating tied for number two. Some individuals use more than one method to manage any side effects so the total number of responses exceed the number of participants. The results are shown in Table 2.13.
To gain some insight into how individuals manage side effects a question was asked regarding the most common methods used. Based on the data 18.6% of participants do not have side effects at all. Lying down came as the primary method with hydration and eating tied for number two. Some individuals use more than one method to manage any side effects so the total number of responses exceed the number of participants. The results are shown in Table 2.13.
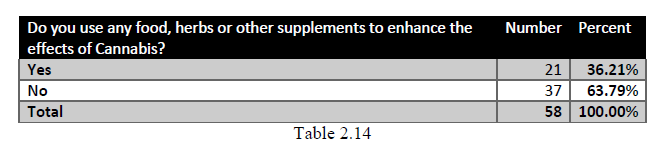
 A question was included to determine if anyone in the survey used food, herbs or other supplements to enhance the effects of cannabis, presumably to reduce their cannabis intake or to improve the condition(s) being treated. The majority of participants or 63.79% claimed that no additional efforts were needed while 21 participants do use something to increase effects. The data is shown in Table 2.14.
A question was included to determine if anyone in the survey used food, herbs or other supplements to enhance the effects of cannabis, presumably to reduce their cannabis intake or to improve the condition(s) being treated. The majority of participants or 63.79% claimed that no additional efforts were needed while 21 participants do use something to increase effects. The data is shown in Table 2.14.
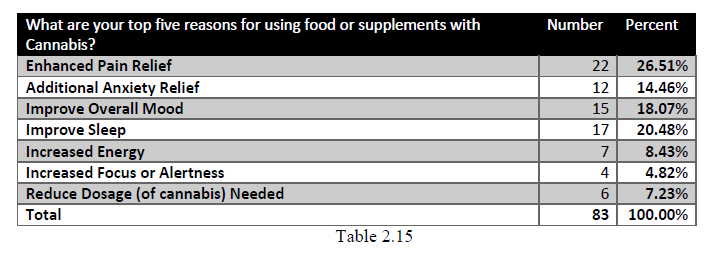
 For those 21 individuals who use methods to enhance the effects of cannabis, a question regarding their stated reasons followed the previous question. The primary answer is to enhance pain relief at 26.51%. Improving sleep, mood and anxiety relief are in second, third and fourth positions respectively. The complete data is shown in Table 2.15.
For those 21 individuals who use methods to enhance the effects of cannabis, a question regarding their stated reasons followed the previous question. The primary answer is to enhance pain relief at 26.51%. Improving sleep, mood and anxiety relief are in second, third and fourth positions respectively. The complete data is shown in Table 2.15.
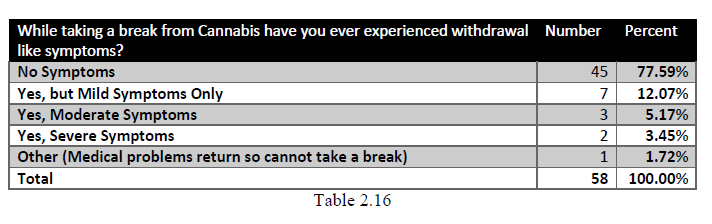
 With phytocannabinoids, withdrawal symptoms are often a matter of intense discussion. In order to determine if these symptoms exist and to what extent a question regarding any symptoms that are withdrawal-like are included in the survey. Of the total number of participants 77.59% indicated that they do not have any such symptoms when taking a break from cannabis. There are 12.07% of respondents indicating only mild symptoms. Three individuals claimed to have moderate symptoms and only two indicated severe symptoms. One person wrote that they have symptoms when taking a break, but clarified that the symptoms experienced is a return of the condition that they are treating with cannabis. See Table 2.16.
With phytocannabinoids, withdrawal symptoms are often a matter of intense discussion. In order to determine if these symptoms exist and to what extent a question regarding any symptoms that are withdrawal-like are included in the survey. Of the total number of participants 77.59% indicated that they do not have any such symptoms when taking a break from cannabis. There are 12.07% of respondents indicating only mild symptoms. Three individuals claimed to have moderate symptoms and only two indicated severe symptoms. One person wrote that they have symptoms when taking a break, but clarified that the symptoms experienced is a return of the condition that they are treating with cannabis. See Table 2.16.
 Since some individuals indicated symptoms with cannabis stoppage, another question was included to determine how long such symptoms last. Interestingly, again, 77.59% claimed no symptoms occur which is additional validation of the previous question. Five responses indicated less than a seven day and only four individual have symptoms lasting longer than one week. The data is found in Table 2.17.
Since some individuals indicated symptoms with cannabis stoppage, another question was included to determine how long such symptoms last. Interestingly, again, 77.59% claimed no symptoms occur which is additional validation of the previous question. Five responses indicated less than a seven day and only four individual have symptoms lasting longer than one week. The data is found in Table 2.17.
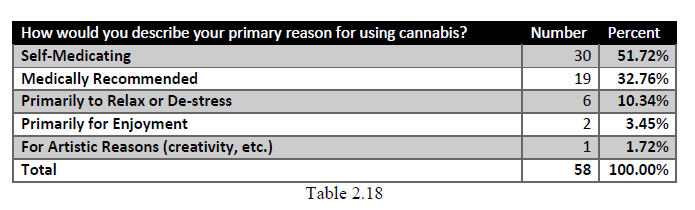
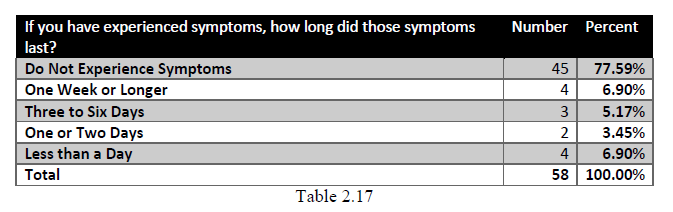 Leading to the thesis of this paper, a question regarding the primary reason for cannabis use is included. A clear 51.72% indicated they are knowingly self-medicating with another 19 individuals or 32.76% using cannabis as medically recommended. This indicates that 84.48% of those surveyed use cannabis for medical reasons whether doing so with a physician’s recommendation or not. Another 10.34% find cannabis helpful to relax or de-stress and only three individuals claimed cannabis use for enjoyment or creativity. The data is shown in Table 2.18.
Leading to the thesis of this paper, a question regarding the primary reason for cannabis use is included. A clear 51.72% indicated they are knowingly self-medicating with another 19 individuals or 32.76% using cannabis as medically recommended. This indicates that 84.48% of those surveyed use cannabis for medical reasons whether doing so with a physician’s recommendation or not. Another 10.34% find cannabis helpful to relax or de-stress and only three individuals claimed cannabis use for enjoyment or creativity. The data is shown in Table 2.18.
 When asked about the individual response to cannabis in terms of overall health, all 58 or 100% of the participants indicated that they “feel better.” Regardless of the medical or “non-medical” reasons stated in the previous question, all of the survey participants clearly indicated that cannabis helps improve their overall sense of wellbeing. See Table 2.19 for the data.
When asked about the individual response to cannabis in terms of overall health, all 58 or 100% of the participants indicated that they “feel better.” Regardless of the medical or “non-medical” reasons stated in the previous question, all of the survey participants clearly indicated that cannabis helps improve their overall sense of wellbeing. See Table 2.19 for the data.
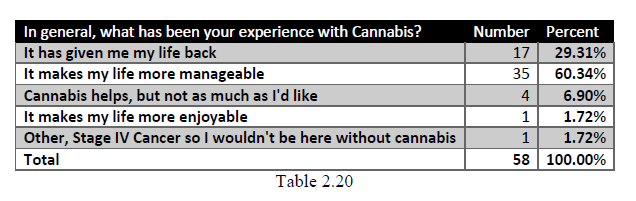
 In order to understand what was meant by “feel better,” a follow-up question asked respondents to reply to a statement that relates closest to their experience. The majority answer was that “it makes my life more manageable,” with 35 choosing this response. The statement “it has given me my life back” came in second with 17 or 29.31%. Four individuals indicated, “Cannabis helps, but not as much as I’d like.” One person noted that “it make my life more enjoyable” with another indicating that they have stage IV cancer and “I wouldn’t be here without cannabis.” See Table 2.20.
In order to understand what was meant by “feel better,” a follow-up question asked respondents to reply to a statement that relates closest to their experience. The majority answer was that “it makes my life more manageable,” with 35 choosing this response. The statement “it has given me my life back” came in second with 17 or 29.31%. Four individuals indicated, “Cannabis helps, but not as much as I’d like.” One person noted that “it make my life more enjoyable” with another indicating that they have stage IV cancer and “I wouldn’t be here without cannabis.” See Table 2.20.
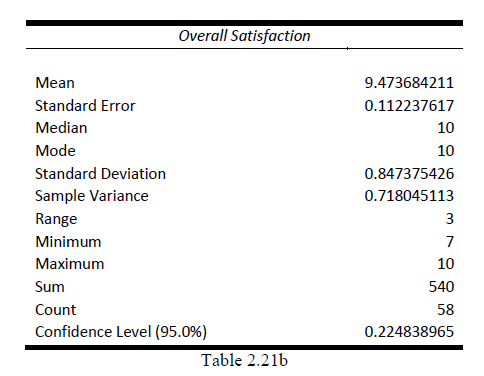
 This last question uses the Likert scale rating from 1-10, with one being the lowest and ten the highest in order to obtain the overall rating of the users experience with cannabis. Of the 58 total participants 65.52% gave cannabis a 10 out of 10 with 22.41% choosing a 9 out of 10, 4 gave it an 8 out of 10, and three gave cannabis a 7 out of 10. See Table 2.21a.
This last question uses the Likert scale rating from 1-10, with one being the lowest and ten the highest in order to obtain the overall rating of the users experience with cannabis. Of the 58 total participants 65.52% gave cannabis a 10 out of 10 with 22.41% choosing a 9 out of 10, 4 gave it an 8 out of 10, and three gave cannabis a 7 out of 10. See Table 2.21a.
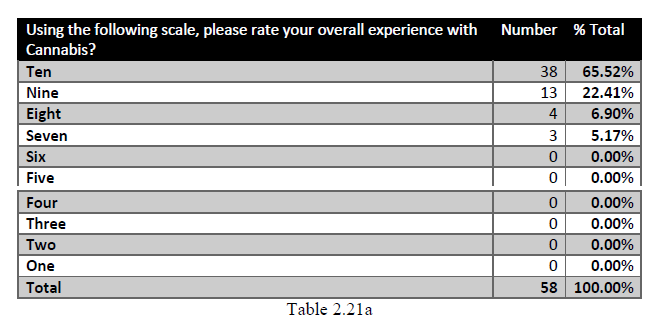 To gain a better understanding of the data from Table 27a, a descriptive analysis was performed on the data in order to obtain the mean, median, mode, standard error, standard deviation and the confidence level to 95%. The mean came in at 9.47, a median and mode of both 10 with a standard deviation of .847 and a confidence level at 95% of .2248. See Table 2.21b for the completed analysis.
To gain a better understanding of the data from Table 27a, a descriptive analysis was performed on the data in order to obtain the mean, median, mode, standard error, standard deviation and the confidence level to 95%. The mean came in at 9.47, a median and mode of both 10 with a standard deviation of .847 and a confidence level at 95% of .2248. See Table 2.21b for the completed analysis.
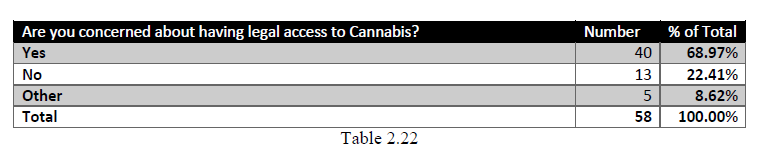
 The last question relates to the concerns of the participants regarding having legal access to cannabis with 68.97% indicating “yes” they are concerned, while 22.41% were not. Another 8.62% offered various answers either due to unavailable cannabis products in legal states or indicating that they would prefer legal access, but will use cannabis whether legal or not. Table 2.22 shows the data.
The last question relates to the concerns of the participants regarding having legal access to cannabis with 68.97% indicating “yes” they are concerned, while 22.41% were not. Another 8.62% offered various answers either due to unavailable cannabis products in legal states or indicating that they would prefer legal access, but will use cannabis whether legal or not. Table 2.22 shows the data.
CASE STUDIES
For the case history reviews, two individuals were selected base on their willingness to participate and their availability. In each case the individual was given an instrument known as the Patient Health Questionnaire or PHQ. The Patient Health Questionnaire (PHQ) is a diagnostic tool for mental health disorders used by health care professionals that is quick and easy for patients to complete. The PHQ is actually a family of screening tools validated in the 1990’s and helps to diagnose five of the most common type of mental disorders primarily represented in medical populations and include depression, anxiety, somatoform, alcohol, and eating disorders. The PHQ-SADS was chosen as the questionnaire for the two case studies since it covers only the depression, anxiety and somatoform symptom scales. The results of the PHQ in the following case history reviews are not to be construed as a diagnosis, but rather a tool to assist in verifying whether one or more of the conditions for which the participants are using cannabis may actually exist. In addition, to protect individual privacy pseudonyms have been used in place of the actual person’s name.
First Case History
The first study participant for a case review is a woman that is in the 25-34 year old age range who we will call Collette. Collette is a single parent with a High School Diploma or GED and is not currently working, but looking for work. In the survey, Collette indicates that she has used cannabis for at least ten years primarily for anxiety, depression, PTSD, and to relax. When asked about her methods of ingestion she prefers smoking or vaping above other methods because of the immediate relief she receives whereas other forms such as edibles or tinctures take typically one to two hours or longer. She could not be certain of the dosages, but estimates that she typically uses about 15-20mg of THC three to four times per day of either a Sativa or an Indica hybrid cultivar. She also uses CBD at a much smaller dose of approximately 3-5mg depending on the plant material available to her. When asked whether she had to increase her dosage from when she first started, she answered “yes”, but has been able to reduce her overall cannabis use over the years. She has experienced some side effects such as anxiety and euphoria primarily with the higher THC sativa cannabis cultivars and either eats food or will lay down to alleviate any unwanted effects. She has not ever experienced severe side effects or withdrawal symptom such as mood changes, irritability, insomnia, headaches, loss of focus, sweating, chills, increased feelings of sadness, or stomach problems when taking a break from cannabis. In the survey, she also answered “yes” when asked if she generally feels better and rates cannabis a 10 out of 10 when asked about her overall experience.
Collette had previously received mental health counseling and fortunately a few of her early medical and psychoeducational evaluations were made available for review, except for the confidential therapeutic notes that were obviously excluded.
According to a 2002 psychoeducational report provided, Collette’s history of emotional distress is first noted around the age of 13, although there are earlier indications of anxiety related to distress at home and may be as a result of her parents’ separation and divorce that occurred two years earlier. A licensed psychologist in private practice first formally evaluated Collette at the age of 14 who noted a marked emotional instability and possibly a mood disorder. Previously she had been placed on Paxil, an SSRI, along with another older Tricyclic drug for depression and anxiety by her regular family medical doctor. It was determined by another family physician that there were contraindications with the two drugs that she was taking at that time. Collette then received both a Psychoeducational Evaluation by the school and subsequently went under the care of a psychiatrist for management of her medication. Collette was moved away from the two contraindicated antidepressants and slowly given newer drug therapies to manage the depression and anxiety. During the next few years, in addition to the pharmaceuticals, Collette received regular psychotherapy and accommodations were made at her school due to the excessive absences to relieve school-related stress. It is noted in the evaluation that the psychiatrist gave her official diagnosis at the time as Depression NOS.
During her teen years, Collette was hospitalized for her “cutting” behavior and an intentional overdose of her prescription medication that required emergency medical care. By the age of eighteen and shortly after her overdose experience, Collette stopped all pharmaceutical medications instead turning to harder “street” drugs as a form of self-medication. She also made the intentional effort of using cannabis to calm herself down. Two or three years later, Collette reports that she was using only cannabis to manage her stress and anxiety and was doing much better. As she reports in the survey, it has worked so well for her she gives cannabis a ten out of ten on effectiveness for her anxiety, depression, PSTD and stress.
To provide clinical evidence of her self-reported answers in the survey, Collette completed the PHQ-SADS that includes the PHQ-9 depression measure, GAD-7 anxiety measure and PHQ-15 for the somatic measure, along with a question regarding panic from the original PHQ. Each section of the PHQ-SADS was scored in order to derive the level of severity for Collette on each of the measures as follows:
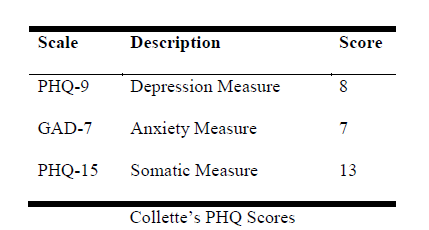 The PHQ-9 depression score falls into the depression severity of mild. Given that Collette has a long history of depression, a result of “mild” is not completely unexpected. Her GAD-7 anxiety scored at seven also falling into the severity category of mild while her PHQ-15 scored at 13, a severity level of moderate. For the questions on anxiety or panic attacks, Collette has not experienced any in several months.
The PHQ-9 depression score falls into the depression severity of mild. Given that Collette has a long history of depression, a result of “mild” is not completely unexpected. Her GAD-7 anxiety scored at seven also falling into the severity category of mild while her PHQ-15 scored at 13, a severity level of moderate. For the questions on anxiety or panic attacks, Collette has not experienced any in several months.
While it is difficult to determine with absolute certainty, Collette does seem to be benefitting from the use of cannabis although the PHQ indicates a ten out of ten is probably a bit optimistic given that she still experiences some mild anxiety and depression. The moderate level on the somatic scale could be related to her diagnosed IBS (irritable bowel syndrome) as she noted in the PHQ that she suffers from nausea, indigestion and stomach pain, which not only increased her score on the somatic measure, but also is often associated with stress and anxiety. While Collette is having success using medical cannabis, during the interview she commented that she typically purchases the least expensive cannabis the dispensary has to offer. This could indicate that she is not getting the correct or best quality medical cannabis for her needs. Overall Collette does feel that using cannabis makes her life more manageable.
Second Case History
The second case study is of a woman in the age range of 55-64 years who we will call Cleo. Cleo has a doctorate degree, but for medical reasons is not working. In the survey, Cleo indicates that she has used cannabis for at least ten years primarily for chronic pain and anxiety. When asked about her methods of ingestion, she currently ingests cannabis in pill or tincture form, but also uses vaping because of the immediate relief she receives whereas other forms take longer for effect. She could not be certain of the dosages for vaping, but indicated that she typically micro-doses twice per day with less than 5mg of a one to one ratio of CBD to THC. Cleo finds that Indica dominant hybrid cultivars work best for her. When asked whether she had to increase her dosage from when she first started, she answered “no,” and has not reduced her overall cannabis use over the years. She experiences euphoria as the primary side effect, but has noticed some anxiety when using a sativa dominant, which is the main reason she now stays with the indica hybrid cultivars. If an unpleasant experience does occur, she finds eating a snack helps with the unwanted effects. She has never experienced severe side effects or withdrawal symptom such as mood changes, irritability, insomnia, headaches, loss of focus, sweating, chills, increased feelings of sadness, or stomach problems when taking a break from cannabis.
Cleo did not have any history of mental health issues and has never been formally diagnosed with a mood or any other mental disorder. However, she did indicate that she was known by close family members as an “anxious” child and has experienced anxiety or panic attacks in the past. She also believes she has PTSD from a traumatic sporting accident that occurred over a decade ago that also left her with chronic pain. In addition to cannabis use, she has engaged in some physical and alternative therapies to help manage the pain as well as the PTSD from the accident.
When asked about her intake, Cleo indicated she started smoking cannabis at the age of 14 and found it helped her to de-stress as well as find creative expression. In the last few years she switched to pills, tinctures and vaping, giving more attention to the type of cannabis and the amount of THC and CBD found in the plant material or extracts. In the survey when asked about the effectiveness of cannabis for her primary conditions, especially anxiety, she gave it 8 out of 10. She also answered “yes” when asked if she generally feels better using cannabis and gave cannabis 10 out of 10 when questioned about her overall experience.
As in the first case study, to provide clinical evidence of Cleo’s self-reported answers in the survey, she completed the PHQ-SADS that includes the PHQ-9 depression measure, GAD-7 anxiety measure and PHQ-15 for the somatic measure, along with a question regarding panic from the original PHQ. Each section of the PHQ-SADS was scored in order to derive the level of severity for Cleo on each of the measures as follows:
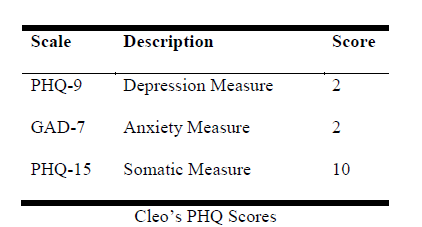
With the PHQ-9 scale Cleo’s score falls into the depression severity of none-minimal. Given that Cleo does not have a history of depression, nor does she think of herself as a “depressed person”, this may be a substantiation of that self-assessment. Her GAD-7 anxiety scoring at two also falls into the category of none-minimal although she has experienced anxiety previously and this her stated reason for moving to Indica dominant cannabis. Her PHQ-15 somatic measure scored at 10 and at a severity level of moderate which may be related to her tendency towards a somaticized expression of anxiety although this is not certain. For the questions on anxiety or panic attacks, Cleo has not experienced any in a few years. Cleo’s self-assessment is in-line with her PHQ-9 scores and indicates that from a therapeutic perspective she is benefitting from cannabis as medicine. In the survey and in the interview Cleo indicated that overall cannabis use makes her life more manageable.
DISCUSSION
In addition to the data derived from this survey in relation to the hypothesis that cannabis is medicine, two other theories are worth mentioning here. Related to the results shown in Table 24, we have the self-medication hypothesis, a theory which was first published in the American Journal of Psychiatry in 1985 (Khantzian, 2017). Athough this theory is postulated in the context of addiction and not directly related to the theory that “cannabis is medicine” as proposed, the notion of self-medication is not completely dissimilar. The difference is that in this study 51.72% of the respondents shown in Table 24 specified that they are self-medicating. The dissimilarity arises in that the participants indicate an awareness of their self-medicating with cannabis and are treating a known health issue themselves without a medical physician’s recommendation. It could be that these individuals self-medicate because it is illegal in their state to obtain medical
cannabis, the public stigma of using an “illegal substance” which often infers an addiction, or possibly these individuals simply prefer a more naturopathic approach to treating their respective conditions.
The second theory is that all cannabis use is medical even when purchased or ingested for non-medical reasons (Macris, 2015). This theory is supported not only by this study and mounting anecdotal evidence, but by published works from both Dr. Bearman and Dr. Sulak who both have written that the ECS is critical in maintaining homeostasis.
Research shows that the human body, when under stress, increases the endocannabinoids in circulation. In other words, endocannabinoid signaling maintains homeostasis when the body is exposed to injury, trauma, stress or exposure to the physiological extremes that result in the activation of the stress response. In fact, one study has shown that acute stress actually increases circulating anandamide even in healthy humans (Dlugos et al., 2012), indicating that this response is a primary role of endocannabinoid signaling. If individuals have an endocannabinoid system that fails to react sufficiently, as proposed by the Endocannabinoid Deficiency Syndrome theory (Russo 2008), then adding phytocannabinoids may be the best answer in helping the individual return to homeostasis. With endocannabinoid deficiency syndrome individuals have a poor ability to buffer stress and this condition is thought to be a contributor to stress-related disorders, such as depression, anxiety, post-traumatic stress disorder and schizophrenia.
Even with the limitations of a small descriptive study, the general notion that cannabis use has medicinal or therapeutic value for those individuals who claim to be using it “recreationally” garners attention especially knowing the important role of the ECS. It can be theorized that one measurement of an individual returning to a more normal healthy state of homeostasis would be a sense of improved health and wellness. When it comes to the survey, the
most relevant questions in support for this theory are 15, 34, 35, 36 and 37. Question 15 directly addresses this idea by asking “How well does cannabis work for your primary condition(s)?” When all the responses are considered, the mean is 8.77193, a high rating on a scale of 1 to 10. Given that only three individuals from question 34 (see Table 24) indicated their primary cannabis use as either for enjoyment or for artistic reasons, question 35 becomes relevant since it additional asks, “Regardless of your primary reason(s) for using cannabis, do you generally feel better?” where 100% of the participants responded “yes.” When underlying possible life stressors are considered, could this mean that these three individuals are also receiving medical benefits? Even if it is presumed that creativity or enjoyment are not related to their stress, it is plausible that ingesting phytocannabinoids may be assisting these individuals’ own endocannabinoid systems.
Looking at the numerous comments from the participants in the study we see clear anecdotal evidence of the medical benefits of cannabis. This first list of excerpts primarily address those comments regarding success in managing pain and other physical illnesses or conditions:
“I have lived with chronic pain for many years. Used to be on pain pills, muscle relaxers, and anti-depressants daily to even be able to sleep half the night. I have cut my meds by 3/4 and feel better just taking cannabis.”
“Using cannabis to treat epilepsy, 98% successful when THC is added to CBD. CBD alone is 80-90% successful, but adding THC gives 98-99% seizure control.”
“I have a debilitating neuromuscular disease called Charcot Marie Tooth disease. I have many other health problems that cause chronic pain. I was hit by a drunk driver causing herniated discs in my neck and lumbar. I have DDD [Depersonalization-Derealization Disorder] and Scoliosis. I prefer Sativa for daytime use to stay alert and be able to function. I use indica at night for pain to sleep better. I hate the euphoria feeling of cannabis, but it helps keep my mind off of my chronic pain. Edibles work well due to the longer lasting effects, but I can control the euphoria better when vaping.”
“I was taking close to 200 Vicodin a month, with cannabis use I was able to cut that down to less than 30 a month.”
“I am a physician who recommends cannabis, primarily for pain and also I use it regularly for my own symptoms of nausea and insomnia.”
“Opiates didn't work well, then high doses of neurontin kinda worked but destroyed my memory. Cannabis has helped me reduce neurontin to 800 mg/day and still function.”
“ CTE) [Chronic Traumatic Encephalopathy] and pain. This is the ONLY medicine I can take for my CTE.”
“I have interstitial cystitis, fibromyalgia, IBS, and hypothyroidism. My bladder pain has significantly reduced. I can now eat many foods I was previously unable to without excruciating pain. Cannabis helps me sleep, and decreases my fibromyalgia pain.”
“I have experienced IBS, diverticulitis, etc., for most of my adult life. While in CO several years ago, I was impressed with the relaxation felt in lower GI as a result of cannabis. Also, the 'high' was excellent and has resulted in a much lower consumption of alcohol. CDB oil is taken at night to aid in sleep. Nice results.”
“I was diagnosed with two degenerating discs in my neck: 5 and 7. The pain traveled to my right arm and numbed my fingers. Tramadol made me feel like a drug addict…Took me 2 weeks to wean from that drug. Spine doctor recommended physical therapy and surgery. I did not want surgery so I researched and learned how to make my own cannabis butter. I no longer have symptoms and the side effect is Cannabis helps me be calm and fall asleep. I do not like smoking because it only lasts 5 minutes for me. Edibles last most the night.”
“The pain I get associated with my monthly cycle is unbearable with cannabis I am able to actually sleep. Nothing has helped before this.”
The following remarks address primarily address mood and related psychopathology, clearly demonstrating the success these individuals have with cannabis use:
“It motivates me to keep focused and get things done, helps me sleep and eat and mellows me out when I'm upset or having an anxiety attack.”
“I struggle with major depressive disorder, social anxiety disorder, and selective mutism. Cannabis has greatly helped me be myself again. I have more energy, motivation, and my mood is better when I consume cannabis every night. I no longer have panic attacks. My depressive episodes are nonexistent. And my overall anxiety is back to healthy levels.”
“I use cannabis to help with my hyper active bipolar and for depression and anxiety.”
“I started out using Cannabis recreationally, but later in life started getting depression and anxiety very intensely, and realized I could use cannabis to help treat those symptoms. That is my main purpose for using Cannabis.”
Many of the same reasons given by the above statements for using cannabis to treat a variety of symptoms are the same as would be offered to a physician who would then prescribe an approved pharmaceutical drug. Here are some examples:
“It makes me relax.” or “It calms me down” – Anxiety or stress. Pharmaceuticals may include Xanax, Klonopin, Valium, Prozac, Cymbalta, Wellbutrin, and the generics.
“It helps me sleep,” Sleep disorder or stress and often prescribed Ambien, Lunesta, or Unisom.
“It helps me to think or be creative.” Likely ADHD or focus and drugs may include Ritalin, Adderall, and Vyvanse.
Taking this concept further; we can look at questions 36 and 37. Question 36, the data for which is found in Table 26 indicates that all the individuals in the survey noticed improvement in their wellbeing with cannabis. Tables 27a and 27b give us data on the overall rating of the individual’s experience with cannabis giving a mean of 9.47 with the median and mode both at 10. This indicates a very high level of satisfaction with the results of cannabis use by all respondents regardless of their reason.
Of course, it is important that we review the matter of side effects and any potential issues with withdrawal symptoms. The side effects noted in this study are euphoria, anxiety, overly sedated or stimulated, nausea, headache, sleeplessness and one person indicating sudden weight gain or loss. However, it is important to put these effects in context. Except for euphoria and sedation, the other six are also found to occur with many traditional pharmaceuticals as well as caffeine, a common substance in coffee, energy drinks, some sodas, and even over-the-counter medication. One researcher, Matthew Lazenka from Virginia Commonwealth University Health System, asserts that cannabis is actually less addictive than drinking coffee (MetroUK, 2015). This is one expert’s opinion, but it is supported by the data found in questions 32 and 33 of this survey.
Looking at Table 22 the data that indicates when the respondents did take a break from cannabis, 91.38% had no or mild withdrawal symptoms with the remaining 8.62% of respondents experiencing moderate to severe symptoms. Table 23 revealed that of those who
experienced such symptoms, 6.9% lasted more than one week. However, no other information about those experiencing long-term effects could be ascertained.
What is known, however, is that the human body has few or no cannabinoid receptors in the lower brainstem areas controlling cardiovascular and respiratory functions, so an “overdose” of cannabis is not lethal (Herkenham et al, 1990). This shows that cannabis is considerably safer with far fewer side effects than prescription opioid drugs, which are known to suppress autonomic functions. Further, as recently reported, two recent studies support the correlation that show a drop in opioid use where cannabis has been legalized (Scientific American, 2018).
There have never been any reports of anyone having died solely from ingesting cannabis at any dose. There have been reports of some unpleasant side effects such as dysphoria and anxiety reported with consumption of high THC products, especially by inexperienced users ingesting edibles.
It is significant that there also appears to be a comorbidity of conditions that individuals are treating with cannabis. Relating to mood, the data indicate high comorbidity of anxiety and depression as well as pain and general mood (both anxiety and depression combined.) In fact, researchers have found that mood disorders, especially depression and anxiety, play an important role in the exacerbation of pain perception in all clinical settings (Woo, 2010). Consequently, the correlation in this study between pain and mood is not surprising. Cannabis does seem to help those individuals suffering from both pain and mood disorders as supported by the data, as further indicated by Cleo in the second case history and by current research.
In terms of treatment, it may be that those who are using cannabis for both pain and mood need to insure they are using the right plant type and profile for their condition and at a therapeutic strength. For example, as anxiety is of concern in the case of Cleo, then Indica
dominant cultivars with a one to one THC:CBD ratio would be recommended since they are less likely to induce anxiety over sativa dominant varieties. However, the dosages would need to be adjusted depending on the individual symptoms and pathology. In the first case history, Collette does appear benefit from cannabis, but as her PHQ scores showed, perhaps not as much as she desired. This may be a result of giving less attention to the type of cannabis plant or product since the financial cost appeared to be a primary driving factor in determining her purchases rather than the quality of the cannabis.
It is also important to observe that according to Cleo, and to an extent inferred by the survey results, side effects such as anxiety are more prevalent with sativa dominant cultivars and high THC products especially in individuals who may have or be prone to anxiety. According to the survey, the number one unwanted side effects that are reported occurred with sativa and high THC use. According to Dr. Bearman in his book titled “Cannabis Medicine” (Bearman & Pettinato, 2018) the preferred proportions for managing pain is a one to one THC to CBD ratio and if anxiety is preexisting, the indica dominant plant or extracts are recommended. Given that there is concern over access to cannabis with 68.97% expressing such a concern, this could contribute to the feeling of apprehension around cannabis use, especially in states where it is still illegal or difficult to access.
What was not considered in this survey and is often overlooked when researching cannabis are the other many cannabinoids and terpenes. Phytocannabinoids such as CBC (Cannabichromene) also act as a pain reliever, and CBC, CBG (Cannabigerol) and CBN (Cannabinol) are all known to aid with sleep. With now over 100 known cannabinoids and over 500 total constituents known to exist in the cannabis plant, much more research needs to be done to examine the role these components play in the alleviation and management of pain and the regulation of mood as well as a host of other health benefits.
Many of the terpenes found in cannabis are also psychoactive, which supports and regulates mood. These terpenes include Myrcene, Limonene, Linalool and Phytol. In addition, Pinene, another terpene, has been found to limit the euphorogenic effects of THC. Using the complete whole plant therapeutically, called the “entourage effect,” may have mitigating properties for some of the unwanted side effects as well as offer additional improvement in treating a variety of medical conditions. This phrase was first used in the cannabis context in 1998 by a group of scientists that included “the father of cannabis research,” renowned Israeli biochemist Dr. Raphael Mechoulam and this concept has been shown to have considerable therapeutic potential beyond the isolated extracts. Therefore it would seem that the entire plant and complete plant extracts (whole plant) are preferable over THC or CBD isolates. (Russo, 2011).
Additionally, the endocannabinoid system is now recognized to play an important role in a number of physiological functions, both in the central and peripheral nervous systems and in peripheral organs. The modulating activity of the endocannabinoid system holds therapeutic promise in a wide range of disparate diseases and pathological conditions. There are numerous studies, in addition to the growing anecdotal evidence, that support cannabis in treating arthritis and neuropathic pain, multiple sclerosis, spinal cord injury, cancer, atherosclerosis, myocardial infarction, stroke, hypertension, glaucoma, obesity/metabolic syndrome, osteoporosis, movement disorders such as Parkinson’s and Huntington’s disease, mood and anxiety disorders, and many other conditions.
STRENGTHS AND LIMITATIONS
The strength of this descriptive study is the detail of information regarding both the length of cannabis consumption and the detail regarding the individual self-assessment of efficacy for the condition or stated purpose of use, including whether the individual achieved a greater overall sense of wellness. An additional strength is that the study provided the opportunity to do follow-up interviews to obtain detailed historical case review and further insight.
This study does have several limitations. The main limitation is the small sample size and limited nature of descriptive surveys generally. This study also relies heavily on self-report questions that may lead to both under-and over-estimates of use and efficacy. Further, because of the illegal nature of cannabis at the federal level in the United States, this illegal status may have affected not only the sample size, but influenced the responses. Certainly this is true when it comes to any identifying information. This may be particularly relevant given that the majority of the respondents are from Utah where cannabis was illegal at the time the study was conducted.
The nature of the study required self-selection and it may be inferred that those who responded could possess a more open-minded approach to the cannabis plant than the general population.
The final limitation concerns the questionnaire used in the survey. Some questions offered multiple responses, which may have confused the intent or clarity of the original question. Further, since the questionnaire was custom no standardizations may be claimed. More specificity on the measurement of cannabis use, e.g. how many times a day, dose, length of use, etc., could not be accurately determined for some methods or types of ingestion. Without a controlled setting and known plant profiles the dosage for smoking and vaping is, at best, a rough estimate so efficacy related to dosage simply cannot be accurately ascertained. The respondents remarks found in the comment section and the case study follow-ups for the two participants do provide more detail and a relevant history of cannabis use than was obtained in the survey adding additional support to the questions asked.
CONCLUSION
With medical cannabis use being legal as of this writing in 33 states, statistical evidence is continuing to expand as more individuals have safe access to the plant. The data from this survey and both of the case studies provide important, although limited, evidence that further supports the claims that cannabis provides human health benefits. Whether or not a person’s sense of well-being is a measure of the human physiology returning to homeostasis, it is probable that if an individual feels better and is experiencing fewer symptoms of an underlying condition that they are treating with cannabis, they likely are healthier.
As Professor Warf (2014) and others have documented, historically cannabis has been used as a medicine by numerous cultures worldwide for thousands of years. Modern science is furthering the understanding of the importance of the entourage effect and perhaps which of the phytocannabinoids, plant terpenes and even alkaloids are the most beneficial to specific diseases. Further research may determine exactly how much of the whole plant or extracts are needed for any health condition. According to Dr. Bearman (2018), the raw whole plant may be the best for overall health because the cannabinoid constituents are found in the form of acids (e.g. THCa, CBDa, etc.) and these acid forms may contain most of the anti-inflammatory, anti-oxidant and other beneficial properties. More research is needed to determine these benefits. In addition, there is less likely to be the euphoric side effects when the fresh plant is juiced or consumed raw. From a practical perspective, juicing or consuming a fresh raw cannabis plant is difficult since most states do not allow growing cannabis at home where the fresh live plant would be most available.
As time goes on, more and more studies are supporting the claims of those who use cannabis for relief from certain conditions such as depression, insomnia and anxiety and, as noted by one study participant, “to stimulate creativity.” It can clearly be reasoned that every participant in this study is using cannabis to manage one or more conditions that are or may have otherwise been treated with pharmaceuticals. This leads us back to the recommendation for health offered by Dr. Sulak (2015) which is to eat a healthy diet, receive sufficient sleep, exercise and additionally consume “whole plant” cannabis in whatever form and dosage is ideal for the individual situation.
CLINICAL IMPLICATIONS
The present study contributes to the existing body of knowledge about the association between cannabis use and improvement in overall health symptoms. This knowledge could be very useful for health care practitioners who are tasked with making medical recommendations for cannabis. It also emphasizes looking beyond the illness or condition being treated and offers focus on the importance of homeostasis in human health presenting as a sense of overall wellness. It would also be valuable to this work if further research could provide direct evidence of the relationship between the blood levels of cannabinoids in the circulation and an individual’s own sense of health and wellness.
Given the nature of this study’s small sample size, I would recommend conducting a significantly larger survey using a standardized version of this or a similar questionnaire where the number of participants was in the hundreds or perhaps thousands. We know that the larger the sample set, the greater the validity of the statistical data. As a result of larger studies, medical research efforts into cannabis might also be expanded since the current classification of cannabis as a Schedule 1 drug has inhibited most potential research in the United States. This would provide additional support to both medical and legal efforts to make cannabis available to more of the population who could benefit from its use.
BIBLIOGRAPHY
Abel, E.L. (1980) Marihuana - The First Twelve Thousand Years. New York: Springer.
Ago, D. C. (2018, August 12). “Cannabis Hyperemesis Syndrome” (CHS) is actually Azadirachtin (neem) poisoning! Retrieved: https://steemit.com/cannabis/@drutter/cannabis-hyperemesis-syndrome-chs-is-actually-azadirachtin-neem-poisoning
All Cannabis Use is Medical, Even if the User Doesn’t Realize it. Halcyon Organics (2015, September 2). Retrieved from: https://halcyonorganics.com/all-cannabis-use-is-medical/
Bearman, David (2008). Medical Marijuana: Scientific Mechanisms and Clinical Indications.
Bearman, David, & Pettinato, M. (2018). Cannabis Medicine: A Guide to the Practice of Cannabinoid Medicine. Santa Barbara, California: Blue Point Books
Bluett, R. J., Gamble-George, J. C., Hermanson, D. J., Hartley, N. D., Marnett, L. J., & Patel, S. (2014). Central anandamide deficiency predicts stress-induced anxiety: behavioral reversal through endocannabinoid augmentation. Translational Psychiatry, 4(7), e408. https://doi.org/10.1038/tp.2014.53
Dincheva, I., Drysdale, A. T., Hartley, C. A., Johnson, D. C., Jing, D., King, E. C., Lee, F. S. (2015). FAAH genetic variation enhances fronto-amygdala function in mouse and human. Nature Communications, 6, 6395.
Dlugos, A., Childs, E., Stuhr, K. L., Hillard, C. J., & de Wit, H. (2012). Acute Stress Increases Circulating Anandamide and Other N-Acylethanolamines in Healthy Humans. Neuropsychopharmacology, 37(11), 2416–2427. https://doi.org/10.1038/npp.2012.100
ECHO. (2017, May 10). What is Clinical Endocannabinoid Deficiency? Retrieved from https://echoconnection.org/clinical-endocannabinoid-deficiency/
ElSohly, M. A. (Ed.). (2006). Marijuana and the Cannabinoids. New Jersey: Humana Press.
Grotenhermen, F., & Müller-Vahl, K. (2012). The Therapeutic Potential of Cannabis and Cannabinoids. Deutsches Ärzteblatt International, 109(29–30), 495–501. https://doi.org/10.3238/arztebl.2012.0495
Herkenham, M., Lynn, A. B., Little, M. D., Johnson, M. R., Melvin, L. S., de Costa, B. R., & Rice, K. C. (1990). Cannabinoid receptor localization in brain. Proceedings of the National Academy of Sciences of the United States of America, 87(5), 1932–1936. https://doi.org/10.1073/pnas.87.5.1932
Hyman, Scott M., & Sinha, R. (2008). Stress-related factors in cannabis use and misuse: Implications for prevention and treatment. Journal of Substance Abuse Treatment, 36 (4), 400-413
Huestis, M. A. (2002). Cannabis (Marijuana) - Effects on Human Performance and Behavior. Forensic Science Review, 14(1–2), 15–60.
Institute of Medicine. (1999). Marijuana and Medicine: Assessing the Science Base. Washington, DC: The National Academies Press. https://doi.org/10.17226/6376
Iversen, L. (2000). The Science of Marijuana. Oxford, New York: Oxford University Press.
Im, J. J., Namgung, E., Choi, Y., Kim, J. Y., Rhie, S. J., & Yoon, S. (2016). Molecular Neuroimaging in Posttraumatic Stress Disorder. Experimental Neurobiology, 25(6), 277–295. https://doi.org/10.5607/en.2016.25.6.277
Kander, J. (2013, October 17). The Comprehensive Report on the Cannabis Extract Movement and the Use of Cannabis Extracts to Treat Diseases. Retrieved from https://www.goodreads.com/work/best_book/27167847-the-comprehensive-report-on-the-cannabis-extract-movement-and-the-use-of
Khantzian, E. J. (2017) The Theory of Self-Medication and Addiction. Psychiatric Times. 34 (2). Retrieved from http://www.psychiatrictimes.com/addiction/theory-self-medication-and-addiction
Kohut, T. (2017, February 5). Teens turn to marijuana to self-medicate for stress, anxiety: report. Global News Canada. Retrieved from https://globalnews.ca/news/3225901/teens-turn-to-marijuana-to-self-medicate-for-stress-anxiety-report/
Korn, L. & MD, Lake, James. (2016). Nutrition Essentials for Mental Health: A Complete Guide to the Food-Mood Connection. New York: W. W. Norton & Company.
Laverty, K. U., Stout, J. M., Sullivan, M. J., Shah, H., Gill, N., Holbrook, L., Bakel, H. (2018). A physical and genetic map of Cannabis sativa identifies extensive rearrangement at the THC/CBD acid synthase locus. Genome Research, gr.242594.118. https://doi.org/10.1101/gr.242594.118
Lloyd, S. L., & Striley, C. W. (2018). Marijuana Use Among Adults 50 Years or Older in the 21st Century. Gerontology and Geriatric Medicine, 4. https://doi.org/10.1177/2333721418781668
McPartland, J. M., Guy, G. W., & Di Marzo, V. (2014). Care and Feeding of the Endocannabinoid System: A Systematic Review of Potential Clinical Interventions that Upregulate the Endocannabinoid System. PLoS ONE, 9(3). https://doi.org/10.1371/journal.pone.0089566
Macris, D. (2015, September 2). All Cannabis Use is Medical, Even if the User Doesn’t Realize it. Halcyon Organics. Retrieved from https://halcyonorganics.com/all-cannabis-use-is-medical/
Mechoulam, R. (Ed.). (2005). Cannabinoids as Therapeutics. Berlin: Birkhäuser.
Medicine, I. of. (1999). Marijuana and Medicine: Assessing the Science Base. https://doi.org/10.17226/6376
MetroUK (2015, April 17) Smoking weed is less addictive than drinking coffee, drug expert claims. Retrieved from: https://metro.co.uk/2015/04/17/smoking-weed-is-less-addictive-than-drinking-coffee-drug-expert-claims-5155336/
Nelson, S. M. (1993). The Archaeology of Korea. United Kingdom: Cambridge University Press.
Onaivi, E. S. (Ed.). (2002). The Biology of Marijuana: From Gene to Behavior. New York: CRC Press.
Patel, S., & Hillard, C. J. (2006). Pharmacological evaluation of cannabinoid receptor ligands in a mouse model of anxiety: further evidence for an anxiolytic role for endogenous cannabinoid signaling. The Journal of Pharmacology and Experimental
Therapeutics, 318(1), 304–311. https://doi.org/10.1124/jpet.106.101287
Patel, S., & Hillard, C. J. (2009). Role of Endocannabinoid Signaling in Anxiety and Depression. Current Topics in Behavioral Neurosciences, 1. https://doi.org/10.1007/978-3-540-88955-7_14
Patient Health Questionnaire (PHQ) Screeners. (2014, December 9). Retrieved from https://www.phqscreeners.com/select-screener
Pertwee, R. G. (Ed.). (2005). Cannabinoids. New York: Springer.
Pertwee, R. (2005). Handbook of Experimental Pharmacology. https://doi.org/10.1007/3-540-26573-2_1
Robson, P. (2001). Therapeutic aspects of cannabis and cannabinoids. British Journal of Psychiatry, 178(2), 107-115. https://doi.org/10.1192/bjp.178.2.107
Russo, E. B. (2008). Clinical endocannabinoid deficiency (CECD): can this concept explain therapeutic benefits of cannabis in migraine, fibromyalgia, irritable bowel syndrome and other treatment-resistant conditions? Neuro Endocrinology Letters, 29(2),
192–200.
Russo, E. B. (2011). Taming THC: potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. British Journal of Pharmacology, 163(7), 1344–1364. https://doi.org/10.1111/j.1476-5381.2011.01238.x
Russo, E. B. (2016). Clinical Endocannabinoid Deficiency Reconsidered: Current Research Supports the Theory in Migraine, Fibromyalgia, Irritable Bowel, and Other Treatment-Resistant Syndromes. Cannabis and Cannabinoid Research, 1(1), 154–165. https://doi.org/10.1089/can.2016.0009
Scientific American (2018, April 2) Where Marijuana Is Legal, Opioid Prescriptions Fall. Retrieved from: https://www.scientificamerican.com/article/where-marijuana-is-legal-opioid-prescriptions-fall/
Strayed, D. C. (2018, October 25). Report: “All Cannabis Use is Medicinal” Whether You Know it Or Not. Retrieved from: http://urhealthinfo.com/2018/10/25/report-all-cannabis-use-s-meicinal-whether-you-know-it-or-not/
Sulak, D. (2015). Introduction to the Endocannabinoid System. NORML.org. Retrieved from https://norml.org/library/item/introduction-to-the-endocannabinoid-system/
The Demographic Statistical Atlas of the United States - Statistical Atlas. (2018). Retrieved from https://statisticalatlas.com/United-States/Educational-Attainment
The National Academies of Sciences, Engineering, and Medicine. (2017). The health effects of cannabis and cannabinoids: Cannabis committee conclusions. Retrieved from https://www.nap.edu/resource/24625/Cannabis_committee_conclusions.pdf
University of Toronto (2018, November 26). How ancient viruses got cannabis high: Ancient viruses contributed to the evolution of hemp and marijuana. Retrieved from: https://www.sciencedaily.com/releases/2018/11/181126105506.htm
Warf, B. (2014). High Points: An Historical Geography of Cannabis. Geographical Review, 104(4), 414–438. https://doi.org/10.1111/j.1931-0846.2014.12038.x
Woo, A. K. (2010). Depression and Anxiety in Pain. Reviews in Pain, 4(1), 8–12. https://doi.org/10.1177/204946371000400103
Zaske, S. Can Marijuana Ease Mental Health Conditions? APA Monitor (2018, December). Retrieved from http://mobileservices.texterity.com/apamonitor/201812/MobilePagedArticle.action?articleId=1444263&lm=1543590456000
ILLUSTRATIONS
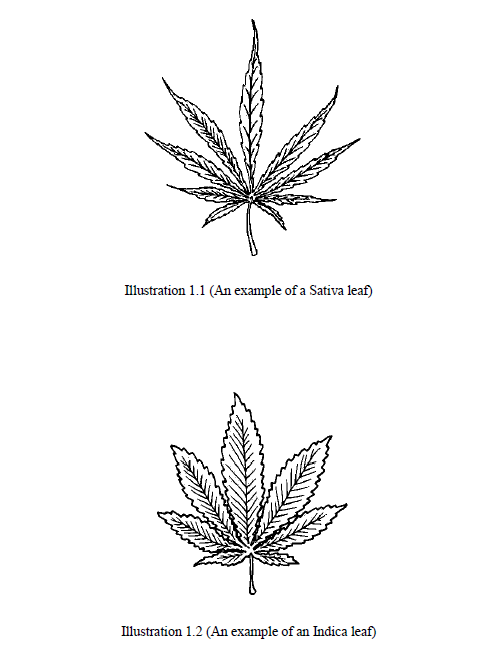
APPENDIX A: ABBREVIATIONS
2-AG 2-Arachidonoyl Glycerol
AEA Arachidonoyl Ethanolamine (Anandamide)
CB1 Endocannabinoid Receptor 1
CB2 Endocannabinoid Receptor 2
CBC Cannbidchromene
CBD Cannabidiol
CBG Cannabigerol
CBN Cannabinol
FAAH Fatty Acid Anhydrase
FBN Federal Bureau of Narcotics
ECS Endocannabinoid System
IBS Irritable bowel syndrome
GABA Gamma-aminobutryic Acid
GAD-7 Generalized Anxiety Score Sheet
MAGL Monoacylglycerol Lipase
NIMH National Institute of Mental Health
PHQ Patient Health Questionaire
PHQ-9 Depression Score Sheet
PHQ-15 Somatic Symptom Score Sheet
THC Tetrahydrocannabinol
THCV Tetrahydrocannabivarin
APPENDIX B: GLOSSARY
2-Arachidonoyl Glycerol (2-AG): An endogenous ligand endocannabinoid of the CB1 receptor.
Acid Form Cannabinoids: Raw and/or freshly harvested cannabis contains cannabinoids in the acid form. This means that they have a carboxyl group. In this acid form such as THCA, CBDA, etc., the cannabinoids are not psychotropic, yet still offer various therapeutic properties when consumed.
Auto-flowering: Unlike other species of cannabis, Cannabis ruderalis enters the flowering stage based on the maturity of the plant, rather than its light cycle. With sativa and indica varieties, it is possible to keep the plant in the vegetative state indefinitely by maintaining a long daylight cycle. Ruderalis, however, will enter the flowering stage regardless of daily light duration and cannabis geneticists today refer to this feature as "auto-flowering".
Azadirachtin: An active component found in the neem plant and more commonly known as Neem Oil. It has been implicated in the condition called cannabis hyperemesis syndrome.
Cannabidiol (CBD): One of over 100 cannabinoids found in cannabis. CBD is often considered the second most common cannabinoid in the plant and has shown benefit for many conditions including autism, epilepsy, anxiety and cancer. It is psychoactive, but is not psychotropic (euphoric). CBD acts as an antagonist to THC thereby reducing the euphorogenic effects of THC through allosteric binding.
Cannabis/Hemp: Hemp is traditional and legally considered distinct from cannabis in that is has .3% or less of THC, although this is not based on botany or science. Technically Hemp and Cannabis are the same plant.
Cannabinoid: Cannabinoids are 21 carbon molecules that either block or stimulate CB1 and/or CB2 receptors. These including primarily: CBC, CBCV, CBD, CBDA, CBDV, CBG, CBGV, CBN, CBV, THC, THCA and THCV and others.
CB1/CB2: These are the two principle human cannabinoid receptors. The CB1 receptors are primarily located on nerve cells in the brain, spinal cord, but they are also found in some peripheral organs and tissues. The CB2 receptors are mainly found in the immune system such as white blood cells, in the tonsils and in the spleen.
Cultivar: A cultivar is a grouping of plants selected for desirable characters that are maintained during propagation and is the most basic classification category of cultivated plants in the International Code of Nomenclature for Cultivated Plants(ICNCP).
Drug: A chemical substance, sometimes including food, which alters the normal state of the mind or body, or is used in the diagnosis or treatment of a disease.
Drug Abuse: The deliberate, non-therapeutic use of a drug, which if measured by dose, frequency, or route of administration proves to be detrimental to the individual either psychologically or physically.
Endocannabinoid System (ECS): All mammals have an ECS and it is essential for homeostasis. It consists, at a minimum, of two neurotransmitters anandamide and 2-AG, two receptors CB1 and CB2, and two enzymes FAAH and MAGL.
Entourage Effect: The totality of the effect of all the therapeutic constituents of the plant acting in concert together.
FAAH: Fatty Acid Anhydrase. The enzyme that metabolizes anandamide.
Indica: One of three varieties of cannabis along with sativa and ruderalis, originally lower in THC and higher in CBD and CBN. Indica plants tend to grow shorter and bushier than the
sativa plants. Indica strains tend to have wide, short leaves with short wide blades. The buds of indica strains tend to be wide, dense and bulky.
MAGL: Monoacylglycerol Lipase. The enzyme that metabolizes 2-AG.
Ruderalis: A is a low-THC subspecies of cannabis which is native to Central and Eastern Europe and Russia. Cannabis ruderalis is smaller than the other subspecies of cannabis growing rarely over two feet in height. The plants have "thin, slightly fibrous stems" with little branching The foliage is typically open with large leaves, reaches maturity much quicker than other species of cannabis typically within a five to seven week period from seed.
Sativa: Sativa is generally a high THC low CBD plant and is one of the three major varieties of cannabis along with Indica and Ruderalis. Sativa has been cultivated throughout recorded history, used as a source of industrial fiber, seed oil, food, recreation, religious and spiritual moods and medicine. The effects of sativa are well known for its cerebral high (euphorogenic) and can treat depression, fatigue, ADD/ADHD, PTSD and other conditions.
Terpene: Terpenes are the most ubiquitous class of molecules in nature with over 20,000 known. These are the aromatic and flavorful aspects of cannabis and found in nearly every other plant on the planet. Terpenes also have medicinal benefits and are used in the aromatherapy industry. Some terpenes with therapeutic value are myrcene, limonene, linalool, and pinene.
THC: Tetrahydrocannabinol (THC) is one of the main cannabinoids along with CBD that are found in the cannabis plant. THC is responsible for the majority of the plants psychotropic or euphorogenic effects. THC has medical benefits including being an analgesic and a tendency to increase appetite.
Trichome: The trichomes are crystalline structures that coat the cannabis plants bract and leaf surfaces. They contain the highest cannabinoid content in the plant.
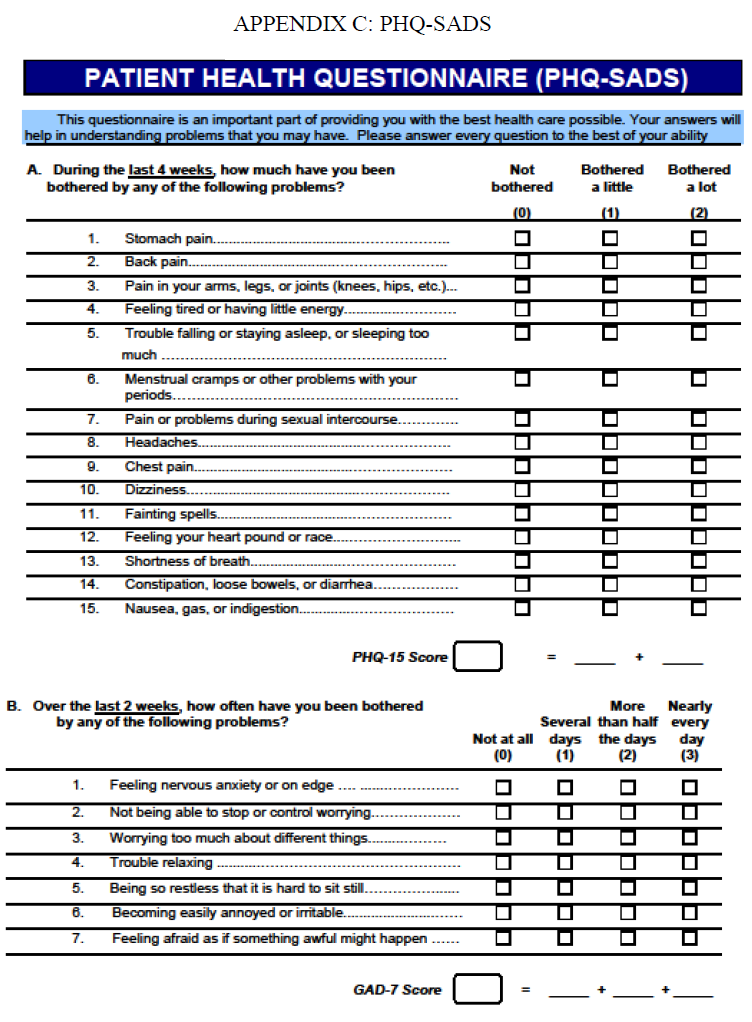
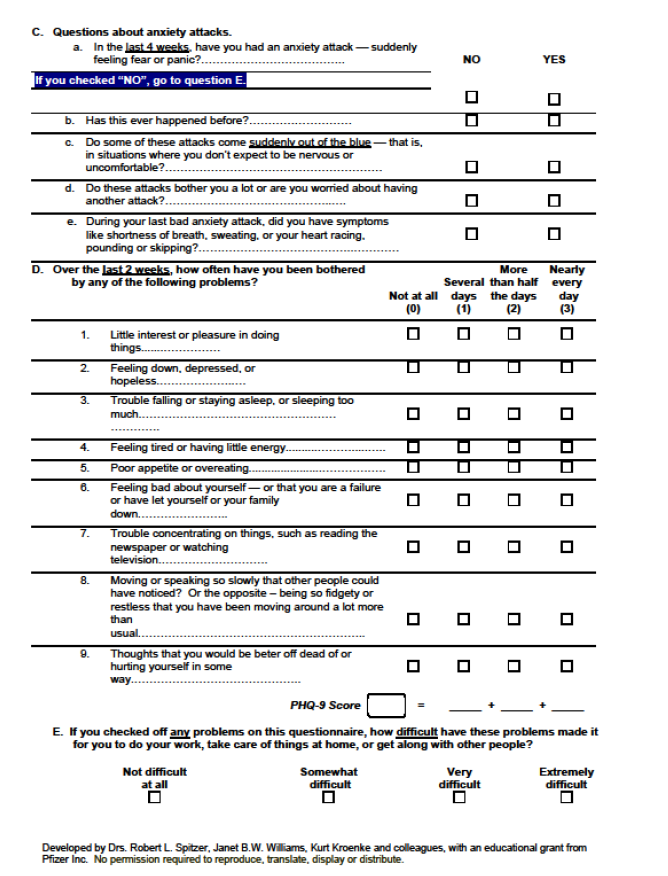
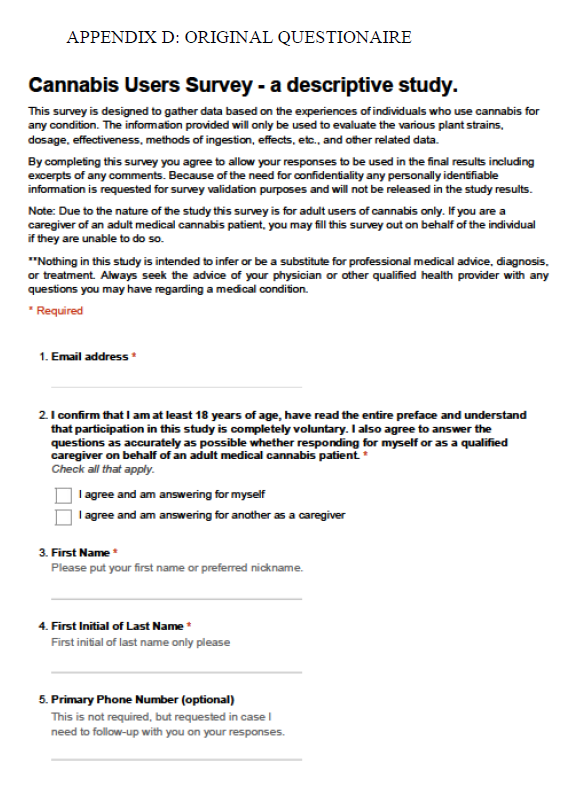
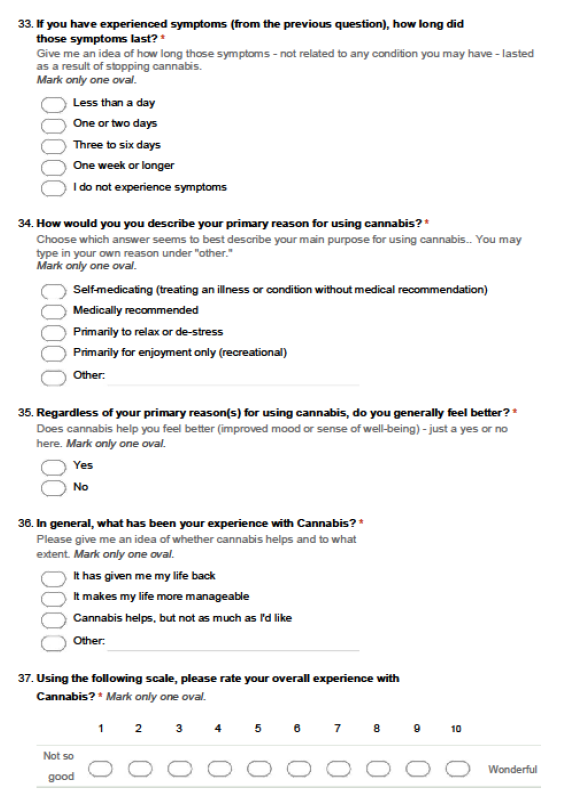
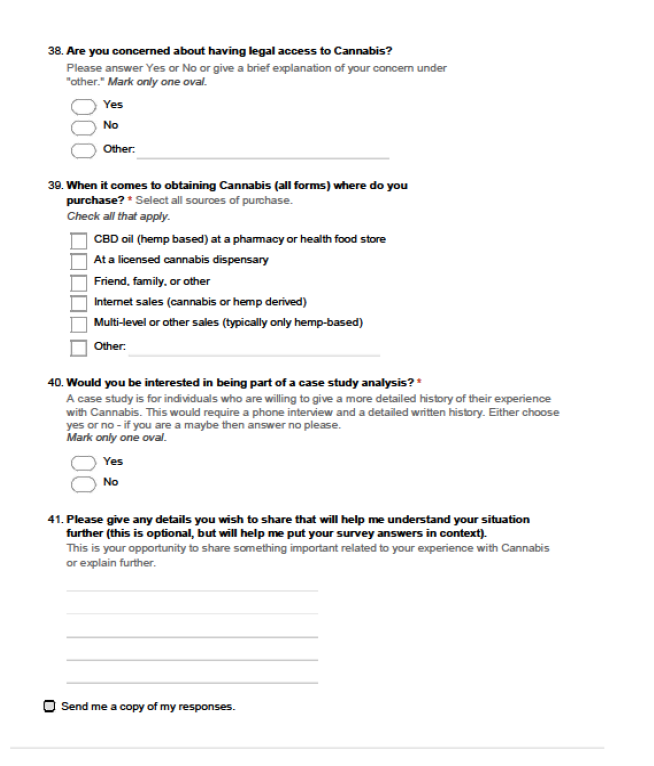
GREAT EDUCATORS HAVE ALWAYS KNOWN THAT LEARNING IS NOT SOMETHING THAT'S LIMITED TO THE CLASSROOMS, OR THAT SHOULD BE FORCIBLY UNDERTAKEN UNDER THE SUPERVISION OF TEACHERS.
BILL GATES
"BEING DOES NOT MEAN ACCEPTING WHAT ONE IS; IT MEANS CREATING ANOTHER SELF THAT DOES NOT EXIST."
J. CHATEAU